Published on
If you are in the early stages of opening or growing your ABA practice, one of the first things you will discover is that families arrive with diagnoses they only partially understand. Global Developmental Delay (GDD) and Autism Spectrum Disorder (ASD) are two of the most commonly conflated diagnoses in early childhood, and confused families make for rocky starts. Learning to distinguish between them, and learning to explain that distinction clearly, is one of the foundational clinical communication skills your practice needs to get right from day one.
Watching a child grow is a thrilling, exhausting, and sometimes tense experience. When families notice their child isn’t hitting the same milestones as peers, they often arrive at a pediatrician’s office hearing terms like Global Developmental Delay or Autism Spectrum Disorder. While these are sometimes mentioned in the same breath, they are entirely different diagnoses, and the distinction shapes everything about how a child should be supported.
In this article, you will explore how global developmental delay and autism are different.
The Core Difference
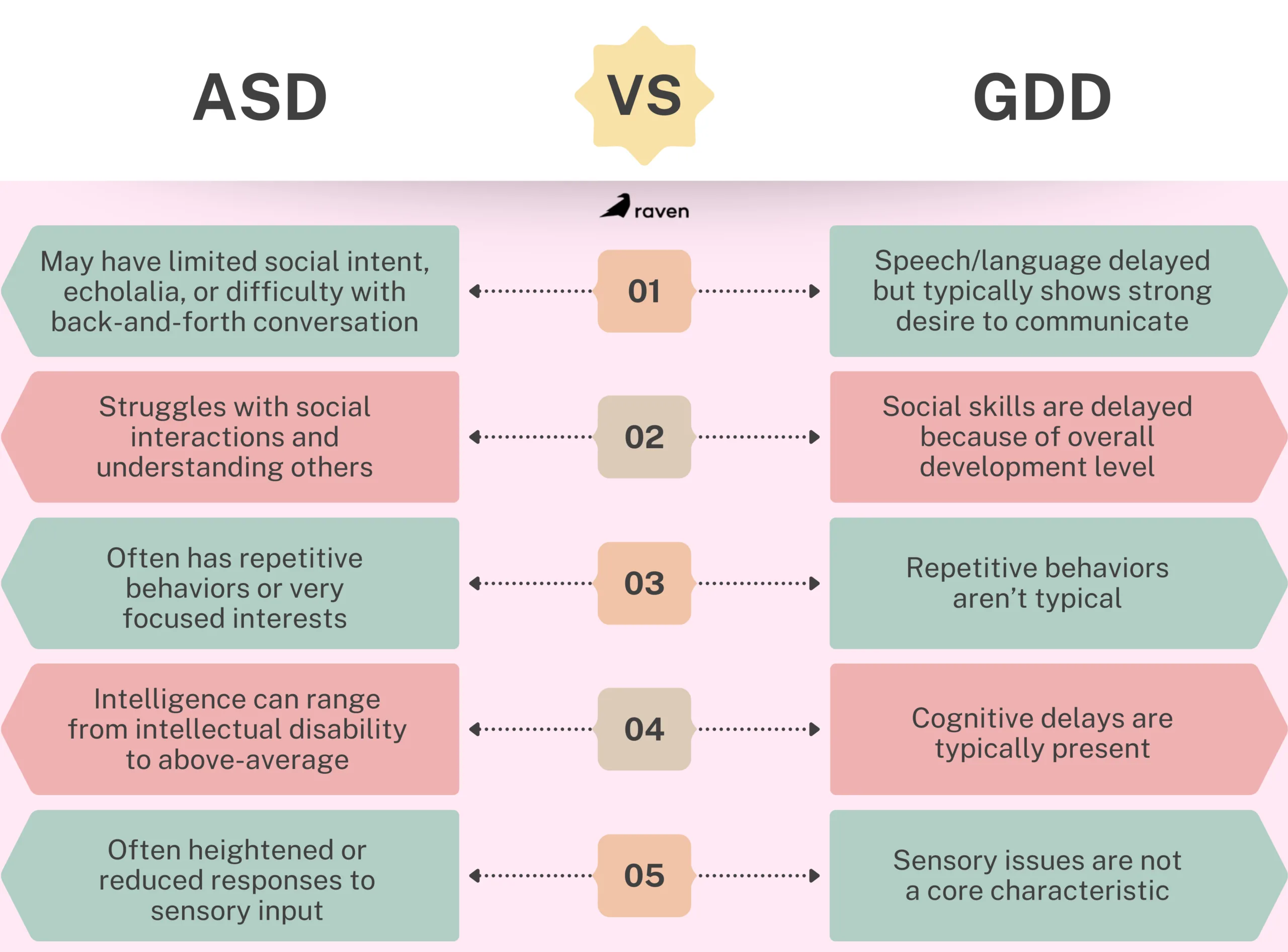
The clearest way to understand the difference between GDD and ASD is to look at the scope of the child’s development.
Global Developmental Delay is exactly what it sounds like: a broad, overarching delay. A child with GDD is significantly lagging behind their peers in at least two or more major developmental domains.
These domains include gross/fine motor skills, speech and language, cognition, social/emotional development, and daily living skills. Think of GDD as a train that is running late on all of its tracks. The child is following the typical path of development; they are just taking longer to get to the stations.
Interestingly, GDD is often considered a temporary or placeholder diagnosis for children under five, as many kids catch up with early intervention, while others might eventually receive a more specific diagnosis like an intellectual disability as they grow older.
Autism Spectrum Disorder, on the other hand, is a specific neurodevelopmental condition. It doesn’t necessarily mean a child is delayed across the board. In fact, a child with ASD might walk early and have an incredible memory for numbers.
Instead, Autism specifically impacts how a person perceives the world and socializes with others. It is characterized by persistent deficits in social communication, coupled with restricted, repetitive patterns of behavior, interests, or activities. If GDD is a train running late, Autism is a train running on a completely different railway system.
It is also worth noting that GDD and ASD are not mutually exclusive. A child can carry both diagnoses simultaneously, and as you design your intake forms and initial assessment protocols, make sure they are built to capture both possibilities rather than assuming a single clean label. Getting this right early prevents misaligned treatment plans that erode family trust before your clinic has had a chance to establish its reputation.
The Gray Area: Where Communication and Behavior Overlap
It is completely understandable why parents and sometimes even professionals initially confuse the two. There is a significant gray area where the symptoms of GDD and ASD overlap, creating a confusing picture for families.
Communication Struggles
Both diagnoses frequently involve speech delays. However, why the child isn’t talking differs. A child with GDD might lack the cognitive or motor skills to form words but will eagerly try to communicate by pointing, making eye contact, or bringing you a toy.
A child with Autism might have the physical ability to speak but lacks the social intent to communicate, or they might struggle to understand the back-and-forth rhythm of a conversation.
Social Hurdles
A child with GDD might seem socially immature simply because they are operating at the cognitive level of a younger child. A child with Autism, however, might actively avoid eye contact, struggle to read facial expressions, or show zero interest in playing with peers, regardless of their cognitive abilities.
Behavioral Meltdowns
Both children can experience severe tantrums. For a child with GDD, meltdowns usually stem from the frustration of not being able to communicate their needs. For an autistic child, meltdowns are frequently sensory-based (the lights are too bright, the room is too loud) or triggered by an unexpected change in routine.
For a new clinic, these overlapping presentations are a reason to slow down during intake rather than speed up. When you and your first BCBAs are still building your assessment rhythm, it is tempting to take a diagnosis at face value and jump into programming. Train your team from day one to document specific behavioral functions and antecedents carefully, because two children with the same diagnosis can need completely different treatment plans. That discipline early on is what separates clinics that get strong outcomes from those that spin their wheels.
How the Evaluation Process Works
You cannot diagnose either of these conditions with a simple blood test. If your pediatrician suspects a delay, they will refer you to a specialist, usually a developmental pediatrician, a pediatric neurologist, or a child psychologist.
The evaluation is a deeply comprehensive, multidisciplinary process.
For Global Delay: Clinicians typically use standardized tests like the Bayley Scales of Infant and Toddler Development. These play-based tests measure the child’s motor, cognitive, and language skills against a massive database of typical peers.
For Autism: The gold standard for an ASD evaluation is the Autism Diagnostic Observation Schedule. This isn’t a test of smarts. It’s an observational tool where the clinician sets up specific social scenarios like a mock birthday party or playing with bubbles to see how the child naturally interacts, requests help, and shares enjoyment.
Clinicians also rely heavily on parent interviews to understand the child’s history and behavior at home. It is also worth noting that a child can actually be diagnosed with both GDD and ASD simultaneously if they meet the criteria for both.
Families often come to a new clinic before a formal evaluation is complete, or with an outdated diagnosis from years prior. As you build out your intake forms, include fields for who conducted the evaluation, when, and what tools were used. This is not bureaucratic overhead. It is the information your BCBA needs to design an accurate treatment plan rather than one built on a label that may no longer reflect where the child actually is. Getting your intake infrastructure right in the first few months of operation saves you from costly clinical misdirection later.
Why Early Identification Matters?
Waiting and seeing is an outdated, risky approach. The human brain is incredibly plastic during the first five years of life, meaning it is exceptionally capable of forming new neural pathways and learning new skills.
Whether your child is diagnosed with a global delay, autism, or both, early identification unlocks the door to Early Intervention (EI) services.
Targeted Therapies
A clear diagnosis ensures the therapies are precise. A child with GDD might need intensive Physical Therapy to learn to walk and Speech Therapy to form words. A child with Autism might benefit more from Occupational Therapy for sensory regulation, or Applied Behavior Analysis (ABA) to build social and adaptive skills.
Empowering the Family
A diagnosis gives you a roadmap. It shifts the narrative from “What is going wrong?” to “Here is how we help.” It connects you with specialized support groups, school accommodations (like an IEP), and state-funded resources.
For a new or growing clinic, early identification is also your most direct path to building a referral pipeline. Developmental pediatricians, early intervention coordinators, and school-based evaluation teams are the first stop for families after a diagnosis, and they refer to clinics they trust. When you demonstrate that your team understands the clinical difference between GDD and ASD, asks the right intake questions, and communicates clearly back to the referring provider, you become the clinic they call first. Prioritize these relationships in your first year of operation. They are your growth engine.
How to Talk to Families About These Diagnoses
In the early days of your clinic, you may be handling much of this family communication yourself before you have a full team in place. Either way, the way your practice talks about these diagnoses shapes how families experience you from the very first conversation. Here is what to build into your communication approach from the start:
- Explain GDD as a starting point, not a permanent ceiling. Many families hear ‘delay’ and assume permanent impairment. Clarifying that GDD is often a placeholder diagnosis and that outcomes depend heavily on early support reduces caregiver anxiety and increases engagement with the treatment plan.
- Reframe the ASD diagnosis as a description, not a limit. Autism describes how a person’s brain processes the world. It does not predict what that person can learn, achieve, or contribute. Families who understand this early are far more motivated partners throughout treatment.
- Use precise language in your clinical documentation from day one. Sloppy language internally leads to sloppy treatment plans. As you onboard your first BCBAs and RBTs, set the expectation that GDD and ASD are documented and discussed as distinct conditions, even when a child has both.
- Position your clinic as a resource, not just a service provider. If a family arrives without a clear diagnosis, guide them toward the evaluation process rather than guessing. New clinics that are honest about what they know and what requires specialist confirmation build credibility faster than those that overreach.
Conclusion
Hearing a diagnosis is incredibly heavy, but it is never the end of your child’s story. It is simply the beginning of getting them the right tools to thrive in their own unique, beautiful way. It acts as a compass. It points families toward the precise therapies, accommodations, and resources that will help the child flourish.
For a new or growing ABA clinic, understanding the distinction between GDD and ASD is not just clinical knowledge. It is the foundation for accurate treatment planning, strong family relationships, and the kind of outcomes that generate the referrals your practice needs to grow.
Get this right from the beginning, and you will not just be a clinic that treats children. You will be a clinic that families and referring providers trust.