Published on

Low-functioning autism represents one of the most complex presentations within the autism spectrum. It is often characterized by significant communication challenges, limited adaptive functioning, and high support needs.
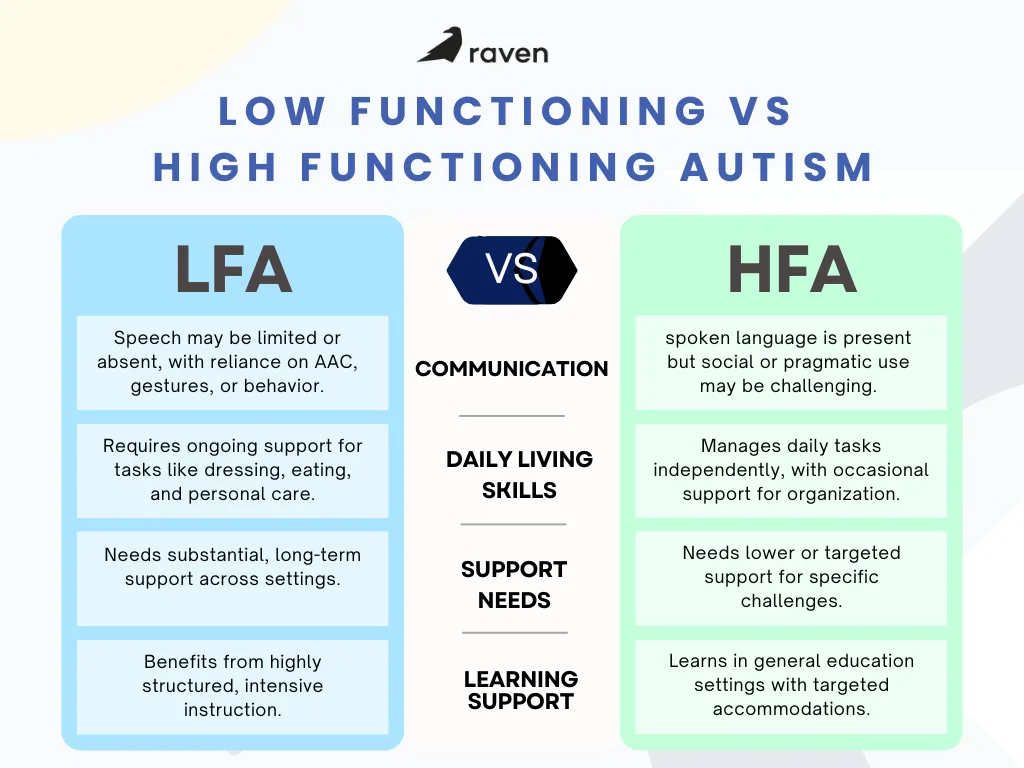
Individuals with low-functioning autism may experience profound difficulties in language development, social engagement, sensory regulation, and daily living skills, requiring consistent, long-term support across home, school, and community settings.
As these individuals transition into adolescence and adulthood, families and healthcare providers frequently face increasing concerns related to independence, safety, and long-term care planning.
In this article, you will explore what low-functioning autism is and the types of support usually needed for individuals with low-functioning autism.
What is Low-Functioning Autism?
Low-functioning autism is a term used to describe individuals on the autism spectrum who have significant support needs, especially in the areas of communication, daily living skills, and behavior regulation. The DSM-5 specifies severity levels for social communication and for restricted, repetitive behaviors to indicate the amount of support required. Level 3 corresponds to requiring very substantial support and often maps clinically to what families call low-functioning autism. Using these levels supports clearer treatment planning.
However, calling someone “low functioning” compresses many different skills into one label and hides individual differences in cognition, communication, motor skills, and adaptive ability. Two people with the same label can have very different profiles, so assessments should be individualized rather than relying on shorthand.
Core Features of Low-Functioning Autism
Individuals with low-functioning autism present the following features:
1. Limited Communication
Individuals with low-functioning autism show marked limitations in spontaneous spoken language. Also, inconsistent functional communication is frequent. When verbal speech is absent or minimal, individuals often rely on gestures, vocalizations, behavior, or alternative communication methods to express needs.
2. Daily Living and Adaptive Skills
Low-functioning autism requires direct teaching and repeated prompting for feeding, dressing, toileting, and other activities of daily living. These skills can require structured, task-analyzed training over long periods and intensive support in home and school settings.
3. Behavior Regulation and Sensory Vulnerability
Severe stress, sensory overload, or unmet needs commonly produce challenging behaviors such as intense meltdown episodes, aggression, self-injury, or elopement. Sensory sensitivities to sound, touch, or visual input often contribute to these reactions and must be evaluated as part of behavior plans.
4. Co-Occurring Medical Conditions
Intellectual disability, epilepsy, sleep disorders, feeding or gastrointestinal problems, and anxiety disorders are reported at higher rates in people with substantial support needs. Routine medical screening and specialist input are essential because untreated medical conditions often worsen behavior.
Support Strategies For Low-Functioning Autism
1. Start with Function
Assessment should identify what the person is trying to accomplish with a behavior. Communication interventions aim to provide a reliable method for requesting, refusing, indicating pain, or gaining attention. Introducing a usable system quickly reduces harm and opens learning time.
2. Augmentative and Alternative Communication
Systematic reviews show AAC approaches, including low-tech picture systems and high-tech speech-generating devices, can increase functional communication and reduce problem behavior when implemented with clear teaching procedures. Implementation fidelity and generalization across contexts are key success factors.
3. Speech and Language Therapy
Therapy should be tailored to current communication skills and pragmatic needs rather than waiting for verbal speech to emerge. Therapists set measurable goals for functional outcomes, such as independent requests for help or clear pain signals.
4. Occupational Therapy
Occupational therapy targets fine motor skills, self-care steps, feeding, and sensory strategies that support participation. Practice should use task breakdown, environmental modification, and graded skills teaching to build independence in daily routines.
5. Behavior Support and Function-Based Planning
Behavior analysis principles are used clinically to identify antecedents, functions, and replacement skills. Interventions teach safer communication alternatives, modify environments, and use positive reinforcement to increase adaptive behaviors while reducing harm. These plans should be multidisciplinary and regularly reviewed.
6. Education and Individualized Programs
Special education services must individualize curricular and daily living goals. Educational plans that include visual schedules, highly structured routines, and supported access to learning produce better engagement and reduce distress in routine transitions.
7. Clinical Indications for Higher Intensity
Intensive programs are most indicated when basic communication is absent, self-care skills are not emerging, or behaviors pose safety risks. Early intensive programs may produce gains in IQ, adaptive behavior, and communication for some children, but responses vary widely and require careful monitoring.
8. Look for Hidden Medical Drivers of Behavior
Pain, constipation, sleep disturbance, seizures, and ear or dental problems frequently present as behavior change. Systematic medical review is standard practice before attributing behavior solely to autism. Treating underlying medical issues often reduces challenging behavior.
Quick Clinical Checklist for Initial Planning
- Confirm diagnosis and document DSM-5 severity levels.
- Complete medical screening for pain, sleep, GI disorders, and seizures.
- Start a functional communication system immediately.
- Define concrete short-term goals for one daily living skill and one safety/behavior target.
- Arrange multidisciplinary review meetings and caregiver training.
Conclusion
People described as having low-functioning autism have substantial, often lifelong support needs in communication, adaptive living, and behavior regulation. Clinical care works best when it is individualized, evidence-informed, and focused first on identifying function, thereby reducing medical contributors to distress and providing a reliable way to communicate.
With structured supports, medical oversight, and team-based planning, clinicians can reduce harm and improve participation and well-being.
Sources:
research.chop.edu/car-autism-roadmap/diagnostic-criteria-for-autism-spectrum-disorder-in-the-dsm-5
psychiatry.org/patients-families/autism/what-is-autism-spectrum-disorder
cdc.gov/autism/about/index.html
pmc.ncbi.nlm.nih.gov/articles/PMC8085719/
research.chop.edu/car-autism-roadmap/diagnostic-criteria-for-autism-spectrum-disorder-in-the-dsm-5
hkjpaed.org/pdf/2020%3B25%3B79-88.pdf
link.springer.com/article/10.1007/s40489-023-00399-x
nice.org.uk/guidance/cg170
ncbi.nlm.nih.gov/books/NBK76942/