Avoid These Common Mistakes When Starting Your ABA Practice
Starting an ABA practice is exciting and full of practical pitfalls. Many new clinics stumble on the same issues that slow growth, hurt cash flow, or risk compliance. In this article, you will explore the most common mistakes that clinics make and practical steps to avoid them.
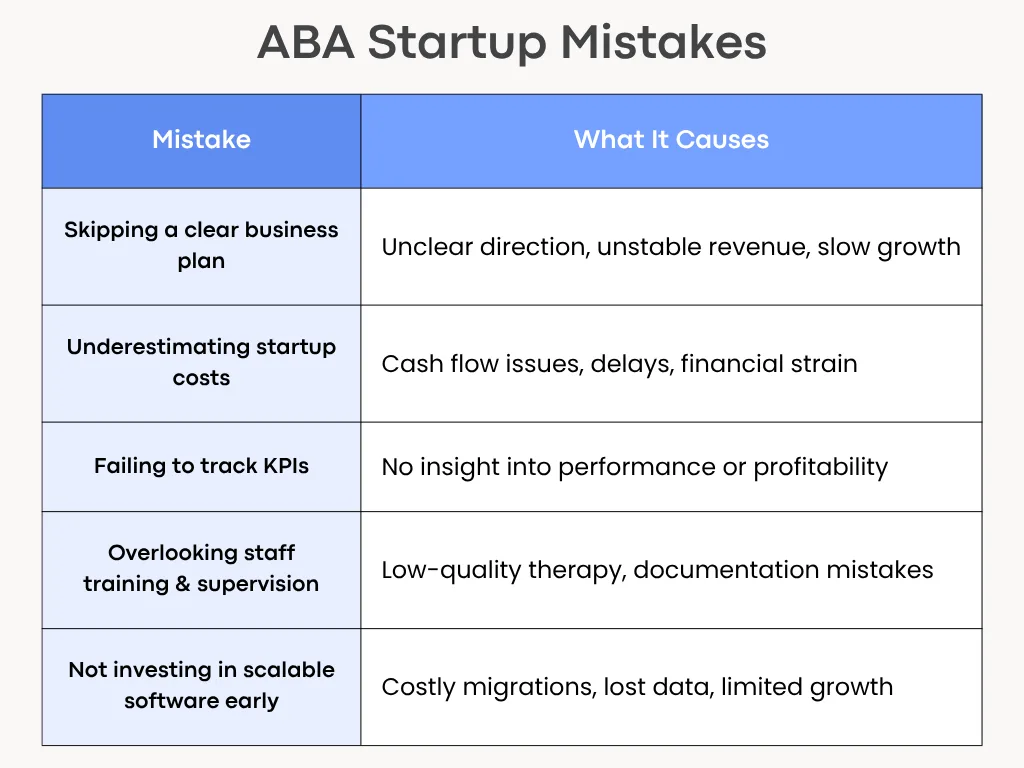
1. Skipping a Clear Business Plan
A good therapy model and strong clinical skills aren’t enough when starting an ABA practice. Without a written business plan, you won’t know who your clients are, how you will get paid, or when the clinic becomes profitable.
What to include in a simple plan?
- Mission and services: Who you serve (age, needs) and which services (intensive ABA, school consultation, tele-health).
- Market and referral sources: schools, pediatricians, insurance panels, and parent groups.
- Revenue model: Typical session rates, payer mix (private pay vs insurance), and expected caseload per clinician.
- Staffing plan: Roles and hires for year 1 and year 2.
- Financial projections: Monthly cash flow forecast for 12 months, break-even date.
- Growth milestones: When to add clinicians, an admin, or a second location.
Write a short one-page plan first and refine it after three months of operations. It’s far easier to adjust a written plan than to improvise under cash pressure.
2. Underestimating Startup Costs
Many founders count only rent and a computer. They miss recurring costs and one-off builds, so cash runs out before the practice stabilizes.
Costs people forget
- Credentialing deposits and payer enrollment fees.
- Billing software, clearinghouse fees, and EMR subscriptions.
- Staff recruitment, background checks, and credential verification.
- Training materials and initial supervision hours for BCBAs.
- Insurance (general liability, professional liability), office supplies, and marketing.
- Working capital to cover payroll for 3–6 months.
Build a conservative budget that includes a three-to-six-month cash buffer. When in doubt, overestimate costs and delay discretionary purchases until revenue is steady.
For more insights, check out our article on ABA startup costs to consider.
3. Delaying Credentialing and Insurance Setup
Credentialing with insurance companies and Medicaid can take months. Waiting to start creates a cash gap and slows patient access.
What to handle early?
- Start payer enrollment as soon as you choose your legal entity and NPI.
- Check state Medicaid requirements and EVV rules if you will bill Medicaid.
- Collect documents up front: provider licenses, malpractice limits, CVs, and contract signatures.
Begin credentialing 90–120 days before you plan to see your first insurance clients. Use a checklist to track submissions and follow-ups weekly.
4. Relying on Paper-Based Data Collection
Paper sheets result in slow supervision, transcription errors, and complicated billing. They also make remote work and audits harder.
Risks of paper
- Lost or illegible session notes.
- Extra admin time to enter data into billing or clinical systems.
- Poor data fidelity for clinical decisions.
Move to a basic digital data-capture tool from day one, even a simple app that syncs to CSV exports. Choose software that supports offline use if you do home visits. Train RBTs on consistent coding and make spot-checks part of supervision.
5. Ignoring Compliance and HIPAA Requirements
HIPAA and state privacy rules are non-negotiable. Gaps expose clients to risk and the clinic to legal and financial trouble.
Key compliance basics
- Sign Business Associate Agreements (BAAs) with any vendor that handles PHI.
- Use encrypted email or a secure portal for families.
- Limit PHI access by role and enable audit logs.
- Keep a breach response plan and test it.
Get BAAs signed before sharing client data. You can use a password manager and MFA for all staff accounts. Also, train staff on privacy rules during onboarding and yearly.
6. Using Disconnected Tools for Billing and Scheduling
Separate systems for scheduling, billing, and charting create manual handoffs, duplicate entry, and missed claims.
Consequences of using disconnected tools
- Billing delays and higher denial rates.
- Frustrated staff who spend time reconciling calendars and notes.
- Hard-to-run reports for utilization or payroll.
Choose an integrated practice management system that fits your budget and workflow. If you can’t afford an all-in-one yet, pick tools with good export/import or API connections and document manual steps to avoid errors.
7. Overlooking Staff Training and Supervision
Good hires aren’t ready without structured onboarding. Undertrained staff make documentation errors and deliver inconsistent therapy.
Elements of strong training
- Role-specific onboarding checklists (RBTs, BCBAs, admin).
- Shadowing and supervised practice blocks before independent caseloads.
- Regular fidelity checks and weekly supervision with documented feedback.
- A clear escalation path for clinical and behavioral emergencies.
Budget for at least 40–80 hours of training per new RBT in the first three months. You can use recorded role-plays and short quizzes to check understanding.
8. Failing to track Key Performance Indicators (KPIs)
Without KPIs you’re guessing whether the business or clinical work is succeeding. Small problems quickly become big.
KPIs to track from day one
- Financial: Days in Accounts Receivable (AR), claim denial rate, net collection rate.
- Clinical: Client attendance rate, average hours per client, and treatment progress by goal.
- Operational: Staff turnover, fill rate for open slots, average time to credential a provider.
Review a short KPI dashboard weekly and a report monthly. Use small experiments (change one thing at a time) and watch the metric move.
9. Neglecting Parent Communication & Collaboration
Parents are partners in therapy. Poor communication hurts retention, progress, and referrals.
What do parents need?
- Clear intake steps and timelines.
- Regular updates: brief weekly notes and a monthly progress snapshot.
- Simple ways to ask questions: portal messages, short phone office hours, or scheduled family meetings.
Send a one-page welcome packet with the treatment plan, goals, who to contact, and what to expect in the first 90 days. Ask for feedback at 30 and 90 days.
10. Not Investing in Scalable Software Early On
Buying the cheapest software that doesn’t scale forces painful migrations later. Data exports, retraining, and process rework cost time and money.
Signs your software won’t scale
- No offline data capture for in-field staff.
- Limited reporting or no API for payroll and billing.
- Difficulty exporting client records in usable formats.
Choose a scalable software like Raven Health that covers core needs (data collection, scheduling, billing, and reporting). Moreover, prioritize exportability and vendor willingness to assist with migration. Consider total cost of ownership, including migration and not just license price.
Conclusion
Many early ABA clinic problems are avoidable with simple, practical planning. Build a short business plan, budget realistically, start credentialing early, and pick scalable digital tools. Train staff well, track key metrics, and keep families part of the process. These steps reduce stress, speed cash flow, and let clinicians focus on what matters most: delivering good care.