Learning a new skill rarely happens in one big leap. Think about how a child learns to tie their shoes; they don’t just watch once and do it. They get stuck, they forget the order, they need someone to guide them through each twist and loop. Applied Behavior Analysis (ABA) recognized this reality long ago, and that’s exactly where chaining comes in.
Chaining is one of those techniques that sounds almost too simple until you actually see it work. It’s a structured way of teaching multi-step skills by breaking them apart and building them back up, one link at a time.
And for many learners, especially those with autism, developmental delays, or other learning differences, it can be genuinely transformative. In this article, you will explore ABA chaining in detail.
What Chaining Actually Is And Why It Matters?
Chaining is a behavior analytic strategy where a complex skill is broken down into its individual behavioral components, each of which can be taught, prompted, and reinforced separately before being connected into a full sequence.
The underlying principle comes from the idea that most meaningful behaviors like washing hands, making a sandwich, getting dressed, aren’t single actions. They’re chains of smaller behaviors where each step acts as both the result of what came before and the signal for what comes next.
In ABA, each step functions as a discriminative stimulus for the next response. What makes chaining so powerful is its precision.
Instead of hoping that a learner will pick it up through observation or general instruction, chaining gives practitioners a clear roadmap. Every step is identified, sequenced, and systematically taught.
Before beginning any chaining program, a task analysis is completed. This typically involves:
Observing someone performing the skill naturally
Breaking the task into the smallest teachable units
Writing each step in observable, measurable terms
Ordering the steps in the sequence they naturally occur
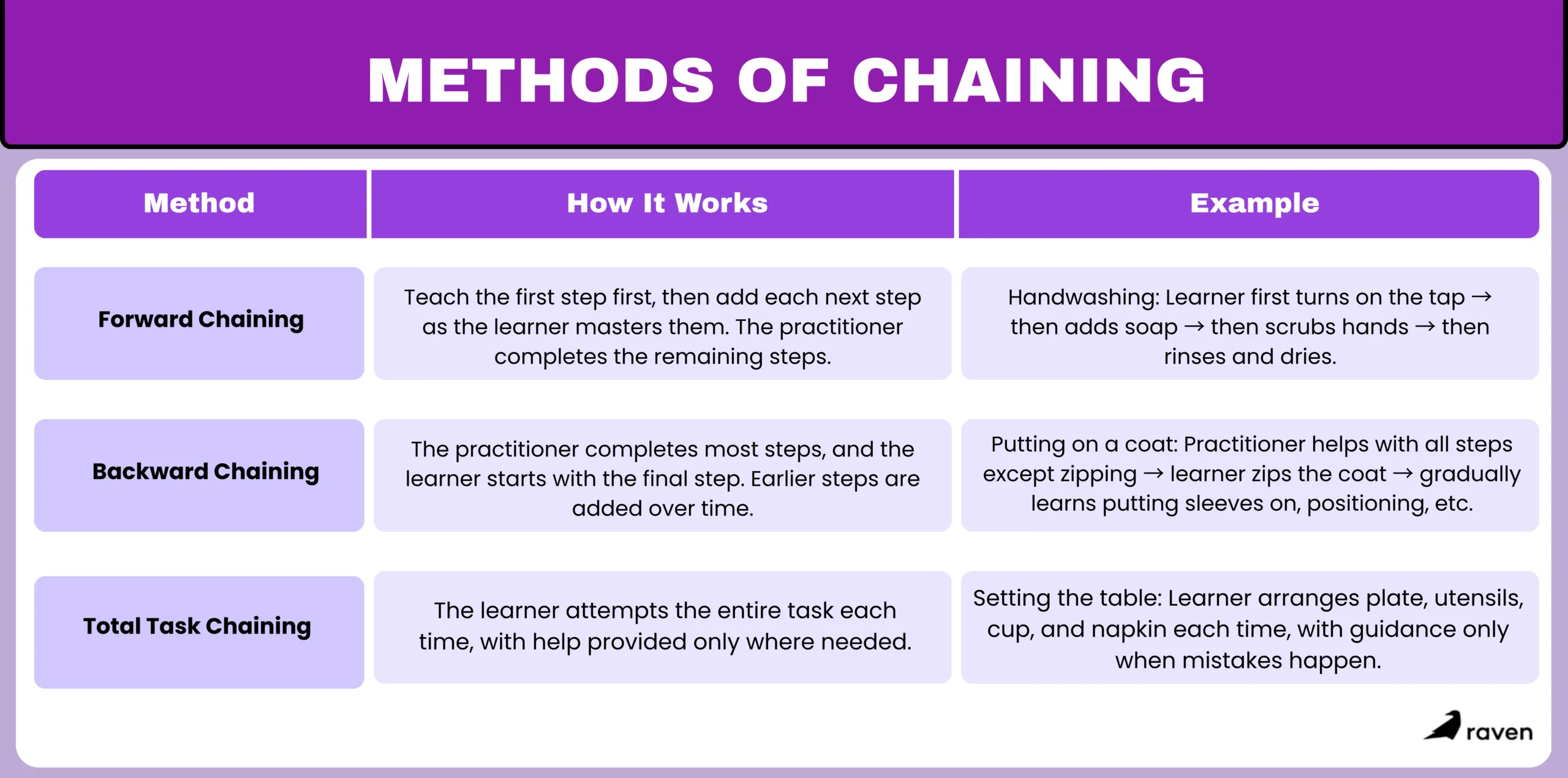
1. Forward Chaining
Forward chaining is exactly what it sounds i.e., teaching the chain from the very first step. The learner is taught step one until they can do it independently, then step two is introduced, and so on.
At each stage, the practitioner provides prompts or completes the remaining steps so the learner can experience the full task from start to finish.
Forward chaining works well when:
The learner is highly motivated by early steps in the sequence
The task has a natural momentum that builds (e.g., assembly tasks)
The beginning steps are the most difficult and need the most practice
The key advantage of forward chaining is early ownership. Since the learner masters and owns the first steps right away, there’s often a stronger sense of progress. They’re not just watching someone else finish the job, they’re contributing from the start.
2. Backward Chaining
Backward chaining flips the script. The practitioner completes all steps except the last one, which the learner performs independently. Once that final step is mastered, the practitioner pulls back to complete all steps except the last two and so on, working backward through the sequence.
This approach has a compelling built-in benefit: the learner always ends the task by completing it. Every single trial result in a finished product, which means reinforcement is consistently delivered at task completion.
Backward chaining is often preferred when:
The final steps of a task are the most naturally rewarding (e.g., eating the completed meal they helped prepare)
The learner needs frequent reinforcement to stay motivated
The practitioner wants to reduce frustration by ensuring task completion every time
Backward chaining is especially well-documented in research with learners who have autism spectrum disorder, where motivation and attention can be real barriers.
3. Total Task Chaining
Total task chaining takes a different approach altogether. Instead of isolating individual steps, the learner attempts the entire chain on every trial, from start to finish. Prompts are provided wherever the learner struggles, and reinforcement is delivered for the completed task.
This method works best in specific circumstances, such as:
The learner already has partial skills across the sequence
The task is relatively short with a small number of steps
The learner does well with full-task practice and doesn’t need step-by-step mastery first.
Think of it like learning to ride a bike with training wheels. You’re doing the whole activity like pedaling, steering, and balancing just with support in the parts you haven’t fully figured out yet. Over time, the support fades.
Total task chaining can be quicker to implement when a learner doesn’t need intensive step-by-step instruction. Research has shown it to be at least as effective as forward or backward chaining in certain populations, though learner characteristics should always guide the decision.
Choosing the Right Type for the Right Learner
There’s no universal answer to which chaining method is best. A good practitioner looks at the learner’s current skill level, what motivates them, the length and complexity of the task, and any history of success or frustration with similar programs.
Forward chaining works best when early steps are the hardest or most motivating. Backward chaining works best when task completion itself is the primary reinforcer. Total task works best for learners with stronger baseline skills or shorter task sequences.
What matters most is that whichever method is chosen, it’s implemented consistently, data is collected at each step, and the program is adjusted based on what the data actually shows. Chaining is a tool, and like any tool, how well it works depends entirely on how it’s used.
Frequently Asked Questions
How do you decide which chaining method to use?
It depends on the learner and the task. Forward chaining is great when early steps are tricky, backward chaining works well when finishing the task is motivating, and total task chaining is ideal when the learner already knows some steps or the task is short.
How do you track progress in ABA chaining?
Progress is tracked by looking at each step of the chain. Notes are taken on whether the learner completes a step independently, needs a prompt, or struggles. This helps guide the next steps and see real improvement over time.
Can chaining be done in a group setting?
Yes. Multiple learners can practice at the same time, each following their own chain. This works well in classrooms or therapy groups where everyone is working on their own skills.
What are common mistakes to avoid with chaining?
Skipping steps, teaching steps out of order, fading prompts too fast or too slow, not tracking progress, or using a method that doesn’t fit the learner can all slow down success.
Conclusion
ABA chaining isn’t a shortcut or a workaround. It’s a carefully structured, evidence-based approach that respects the complexity of real-world skills while meeting learners exactly where they are.
Whether a child is learning to brush their teeth or an adult is working toward independent meal preparation, chaining builds competence piece by piece until one day, the whole chain clicks together without any prompts at all. That moment when a skill becomes truly independent is what all the careful work is for.
As a new ABA clinic owner, you are responsible not just for clinical outcomes but for the quality and consistency of the interventions your team delivers. Response cost is one of those procedures that shows up frequently in treatment plans but gets misapplied just as frequently, especially in newer clinics where supervision structures are still being built.
Understanding it deeply, knowing when it is appropriate, and making sure your BCBAs and RBTs are using it correctly is part of running a clinically sound practice.
Think about the last time you got a speeding ticket. You were driving a little too fast, saw the flashing lights in your rearview mirror, and ended up having to pay a hefty fine. You lost money that you already had in your bank account because of a specific rule violation.
Chances are, the next time you drove down that exact stretch of road, you checked your speedometer. That speeding ticket is a perfect, everyday example of a behavioral concept known as Response Cost.
In the field of Applied Behavior Analysis (ABA), response cost is a highly specific, effective, but delicate tool. When used correctly, it helps individuals understand boundaries and consequences. When used poorly, it can cause frustration and resentment.
In this article, you will explore what this strategy looks like in a clinical or educational setting and how to use it fairly.
What Exactly is Response Cost?
In behavioral terms, response cost is defined as the removal of a specific, previously earned reinforcer immediately following an inappropriate behavior, with the ultimate goal of decreasing that behavior in the future.
Technically speaking, it falls under the category of negative punishment.
Negative means we are taking something away (subtracting).
Punishment means the ultimate effect is that the target behavior happens less often.
It is crucial not to confuse this with negative reinforcement. We aren’t taking away a chore to reward a kid for doing well; we are taking away a prized possession (like a token, a few minutes of recess, or points) because a boundary was crossed. The individual “pays a cost” for their response.
For your clinical team, the distinction between negative punishment and negative reinforcement is one of the most commonly confused concepts in ABA. If you are onboarding new RBTs or BCBAs, it’s vital to ensure this distinction is explicitly covered in your training protocols. Misunderstanding the mechanism means misapplying the procedure.
How It Works?
Response cost is most effective when it is highly concrete. The learner needs to clearly see the connection between what they did and what they lost. Here is what it looks like across different scenarios:
The Classic Token Economy
A child earns a star on their token board for every 10 minutes they stay seated during math class. By the end of the hour, they have five stars, which they can trade in for iPad time. However, if they throw a pencil at a classmate, the teacher immediately removes one star. The cost of throwing the pencil was one star.
The Sibling Dispute
Two teenagers are told that if they finish their chores, they can share the family car on Friday night. They do the chores and earn the car keys. But on Thursday, they get into a massive, screaming fight that breaks a house rule. The parents take the keys back.
The “Time” Penalty
A student earns 15 minutes of extra recess for completing their spelling test early. Later in the day, they refuse to line up when the bell rings. The teacher deducts 2 minutes from their earned recess time.
In a clinic setting, the token economy example is the most common application you will see on treatment plans. As a clinic owner, make sure your BCBAs are documenting the specific response cost parameters in writing, including what behavior triggers the cost, exactly how much is removed, and how the learner can continue earning.
Vague implementation is one of the most common reasons response cost fails and one of the first things an auditor or supervisor will flag.
When is it Appropriate to Use?
Modern ABA heavily prioritizes positive reinforcement. We always want to focus on teaching a child what to do, rather than just punishing them for what they do wrong. Because response cost is a punishment procedure, it should never be your first line of defense.
It is generally appropriate to introduce only after positive reinforcement strategies have been tried and when a behavior remains stubborn or disruptive.
If you and your clinical team decide to implement response cost, there are strict ethical and practical guidelines you need to follow to make sure it is fair:
1. You Must Have a Rich Environment: You cannot take away what a child doesn’t have. If a learner rarely earns tokens, losing one is devastating. Response cost only works if the child is earning reinforcers frequently and easily for good behavior. The ratio of earning to losing should be heavily tilted toward earning.
2. Avoid the Bankruptcy Trap: This is the most common mistake parents and teachers make. If a child starts the day with 5 tokens and loses all 5 by 10:00 AM because of a rough morning, they are bankrupt. At that point, why should they behave for the rest of the day? They have nothing left to lose. Always ensure there is a way for the learner to earn back what they lost, or cap the penalties so they never hit absolute zero.
3. No Surprise Fees: Transparency is everything. The rules must be explicitly clear before the behavior happens. A learner should never be shocked that they lost a token. If the rule is “hitting costs one token,” that rule needs to be stated visually or verbally ahead of time. You cannot make up a penalty in the heat of the moment just because you are frustrated.
As a clinic owner, these three guidelines are also your supervision checklist. If you are observing a session or reviewing session notes and you notice a response cost procedure being applied inconsistently, to a learner with a thin reinforcement history, or without prior disclosure, those are red flags that require immediate BCBA intervention.
Inconsistent application of punishment procedures is both clinically harmful and an ethical violation under the BACB guidelines your team is bound by.
Conclusion
When we introduce a cost for certain actions, we are mimicking how the real-world works. Society runs on a system of earning and losing, whether it is money, privileges, or trust. By implementing response cost thoughtfully, clearly, and fairly, we help learners understand accountability without sacrificing their dignity or their motivation to try again.
For a new or growing ABA clinic, the clinical quality of procedures like this one is inseparable from your reputation. Families talk to each other. Referring providers pay attention to outcomes. The clinics that build strong supervision structures around procedures like response cost from the beginning are the ones that earn trust quickly and keep it.
If you are in the early stages of opening or growing your ABA practice, one of the first things you will discover is that families arrive with diagnoses they only partially understand. Global Developmental Delay (GDD) and Autism Spectrum Disorder (ASD) are two of the most commonly conflated diagnoses in early childhood, and confused families make for rocky starts. Learning to distinguish between them, and learning to explain that distinction clearly, is one of the foundational clinical communication skills your practice needs to get right from day one.
Watching a child grow is a thrilling, exhausting, and sometimes tense experience. When families notice their child isn’t hitting the same milestones as peers, they often arrive at a pediatrician’s office hearing terms like Global Developmental Delay or Autism Spectrum Disorder. While these are sometimes mentioned in the same breath, they are entirely different diagnoses, and the distinction shapes everything about how a child should be supported.
In this article, you will explore how global developmental delay and autism are different.
The Core Difference
The clearest way to understand the difference between GDD and ASD is to look at the scope of the child’s development.
Global Developmental Delay is exactly what it sounds like: a broad, overarching delay. A child with GDD is significantly lagging behind their peers in at least two or more major developmental domains.
These domains include gross/fine motor skills, speech and language, cognition, social/emotional development, and daily living skills. Think of GDD as a train that is running late on all of its tracks. The child is following the typical path of development; they are just taking longer to get to the stations.
Interestingly, GDD is often considered a temporary or placeholder diagnosis for children under five, as many kids catch up with early intervention, while others might eventually receive a more specific diagnosis like an intellectual disability as they grow older.
Autism Spectrum Disorder, on the other hand, is a specific neurodevelopmental condition. It doesn’t necessarily mean a child is delayed across the board. In fact, a child with ASD might walk early and have an incredible memory for numbers.
Instead, Autism specifically impacts how a person perceives the world and socializes with others. It is characterized by persistent deficits in social communication, coupled with restricted, repetitive patterns of behavior, interests, or activities. If GDD is a train running late, Autism is a train running on a completely different railway system.
It is also worth noting that GDD and ASD are not mutually exclusive. A child can carry both diagnoses simultaneously, and as you design your intake forms and initial assessment protocols, make sure they are built to capture both possibilities rather than assuming a single clean label. Getting this right early prevents misaligned treatment plans that erode family trust before your clinic has had a chance to establish its reputation.
The Gray Area: Where Communication and Behavior Overlap
It is completely understandable why parents and sometimes even professionals initially confuse the two. There is a significant gray area where the symptoms of GDD and ASD overlap, creating a confusing picture for families.
Communication Struggles
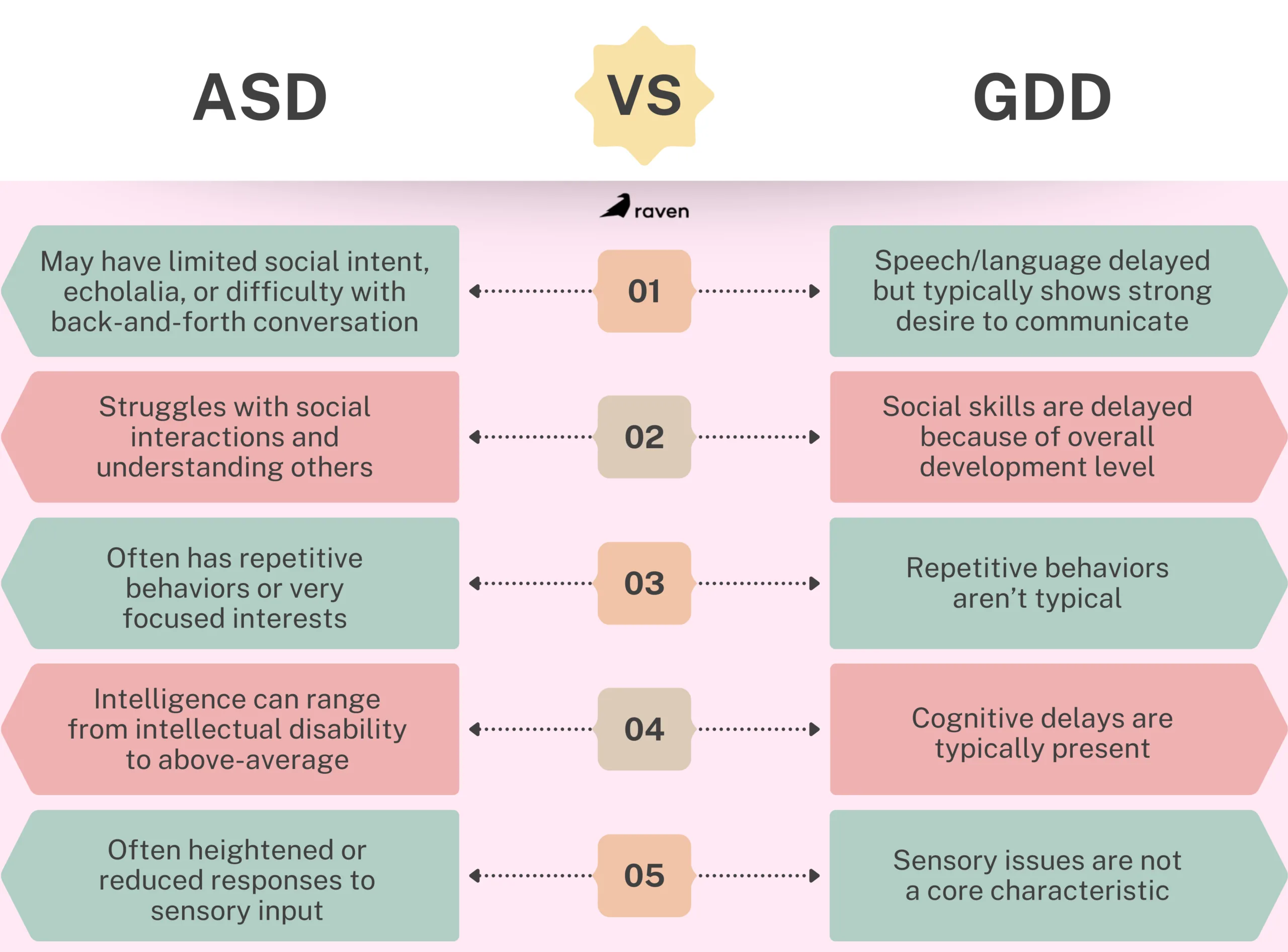
Both diagnoses frequently involve speech delays. However, why the child isn’t talking differs. A child with GDD might lack the cognitive or motor skills to form words but will eagerly try to communicate by pointing, making eye contact, or bringing you a toy.
A child with Autism might have the physical ability to speak but lacks the social intent to communicate, or they might struggle to understand the back-and-forth rhythm of a conversation.
Social Hurdles
A child with GDD might seem socially immature simply because they are operating at the cognitive level of a younger child. A child with Autism, however, might actively avoid eye contact, struggle to read facial expressions, or show zero interest in playing with peers, regardless of their cognitive abilities.
Behavioral Meltdowns
Both children can experience severe tantrums. For a child with GDD, meltdowns usually stem from the frustration of not being able to communicate their needs. For an autistic child, meltdowns are frequently sensory-based (the lights are too bright, the room is too loud) or triggered by an unexpected change in routine.
For a new clinic, these overlapping presentations are a reason to slow down during intake rather than speed up. When you and your first BCBAs are still building your assessment rhythm, it is tempting to take a diagnosis at face value and jump into programming. Train your team from day one to document specific behavioral functions and antecedents carefully, because two children with the same diagnosis can need completely different treatment plans. That discipline early on is what separates clinics that get strong outcomes from those that spin their wheels.
How the Evaluation Process Works
You cannot diagnose either of these conditions with a simple blood test. If your pediatrician suspects a delay, they will refer you to a specialist, usually a developmental pediatrician, a pediatric neurologist, or a child psychologist.
The evaluation is a deeply comprehensive, multidisciplinary process.
For Global Delay: Clinicians typically use standardized tests like the Bayley Scales of Infant and Toddler Development. These play-based tests measure the child’s motor, cognitive, and language skills against a massive database of typical peers.
For Autism: The gold standard for an ASD evaluation is the Autism Diagnostic Observation Schedule. This isn’t a test of smarts. It’s an observational tool where the clinician sets up specific social scenarios like a mock birthday party or playing with bubbles to see how the child naturally interacts, requests help, and shares enjoyment.
Clinicians also rely heavily on parent interviews to understand the child’s history and behavior at home. It is also worth noting that a child can actually be diagnosed with both GDD and ASD simultaneously if they meet the criteria for both.
Families often come to a new clinic before a formal evaluation is complete, or with an outdated diagnosis from years prior. As you build out your intake forms, include fields for who conducted the evaluation, when, and what tools were used. This is not bureaucratic overhead. It is the information your BCBA needs to design an accurate treatment plan rather than one built on a label that may no longer reflect where the child actually is. Getting your intake infrastructure right in the first few months of operation saves you from costly clinical misdirection later.
Why Early Identification Matters?
Waiting and seeing is an outdated, risky approach. The human brain is incredibly plastic during the first five years of life, meaning it is exceptionally capable of forming new neural pathways and learning new skills.
Whether your child is diagnosed with a global delay, autism, or both, early identification unlocks the door to Early Intervention (EI) services.
Targeted Therapies
A clear diagnosis ensures the therapies are precise. A child with GDD might need intensive Physical Therapy to learn to walk and Speech Therapy to form words. A child with Autism might benefit more from Occupational Therapy for sensory regulation, or Applied Behavior Analysis (ABA) to build social and adaptive skills.
Empowering the Family
A diagnosis gives you a roadmap. It shifts the narrative from “What is going wrong?” to “Here is how we help.” It connects you with specialized support groups, school accommodations (like an IEP), and state-funded resources.
For a new or growing clinic, early identification is also your most direct path to building a referral pipeline. Developmental pediatricians, early intervention coordinators, and school-based evaluation teams are the first stop for families after a diagnosis, and they refer to clinics they trust. When you demonstrate that your team understands the clinical difference between GDD and ASD, asks the right intake questions, and communicates clearly back to the referring provider, you become the clinic they call first. Prioritize these relationships in your first year of operation. They are your growth engine.
How to Talk to Families About These Diagnoses
In the early days of your clinic, you may be handling much of this family communication yourself before you have a full team in place. Either way, the way your practice talks about these diagnoses shapes how families experience you from the very first conversation. Here is what to build into your communication approach from the start:
Explain GDD as a starting point, not a permanent ceiling. Many families hear ‘delay’ and assume permanent impairment. Clarifying that GDD is often a placeholder diagnosis and that outcomes depend heavily on early support reduces caregiver anxiety and increases engagement with the treatment plan.
Reframe the ASD diagnosis as a description, not a limit. Autism describes how a person’s brain processes the world. It does not predict what that person can learn, achieve, or contribute. Families who understand this early are far more motivated partners throughout treatment.
Use precise language in your clinical documentation from day one. Sloppy language internally leads to sloppy treatment plans. As you onboard your first BCBAs and RBTs, set the expectation that GDD and ASD are documented and discussed as distinct conditions, even when a child has both.
Position your clinic as a resource, not just a service provider. If a family arrives without a clear diagnosis, guide them toward the evaluation process rather than guessing. New clinics that are honest about what they know and what requires specialist confirmation build credibility faster than those that overreach.
Conclusion
Hearing a diagnosis is incredibly heavy, but it is never the end of your child’s story. It is simply the beginning of getting them the right tools to thrive in their own unique, beautiful way. It acts as a compass. It points families toward the precise therapies, accommodations, and resources that will help the child flourish.
For a new or growing ABA clinic, understanding the distinction between GDD and ASD is not just clinical knowledge. It is the foundation for accurate treatment planning, strong family relationships, and the kind of outcomes that generate the referrals your practice needs to grow.
Get this right from the beginning, and you will not just be a clinic that treats children. You will be a clinic that families and referring providers trust.
When you are in the early stages of building an ABA practice, every tool you adopt becomes part of your foundation. Choosing the wrong practice management system does not just create headaches later, it slows your ability to take on clients, bill cleanly, and retain staff. That is why the demo stage matters more for a new or growing clinic than for an established one. You are not evaluating whether to replace something. You are deciding what to build on.
If you run a growing ABA clinic, you already know the software struggle. Clinicians burn out not from the therapy itself, but from the clunky, outdated technology they are forced to use to document it. When your Registered Behavior Technicians (RBTs) spend more time fighting a loading screen than engaging with their learners, your entire operational flow breaks down. Raven Health has emerged as a strong alternative in the ABA practice management space, specifically targeting the everyday frustrations of data collection and clinical documentation. But before committing your entire staff to a new platform, you need to first see it in action.
Here is exactly what you can expect during a Raven Health demo, who should be on the call, and how to best use that time to figure out if it is the right fit for where your practice is headed.
Who is The Demo For?
A common mistake clinics make when evaluating new software is only having the owner or a single administrator watch the demo. Raven Health is an end-to-end platform, meaning it touches every level of your organization. If your organization is small, it is worth thinking about this demo through the lens of each role you will eventually need to fill.
And if you are a solo owner who is also acting as your own BCBA, administrator, and billing contact, use Raven’s demo to think in layers: watch it through the lenses of a clinician, as an operations person, and as a person responsible for getting your team paid. Ask questions from all three angles.
1. Clinic Owners and Directors
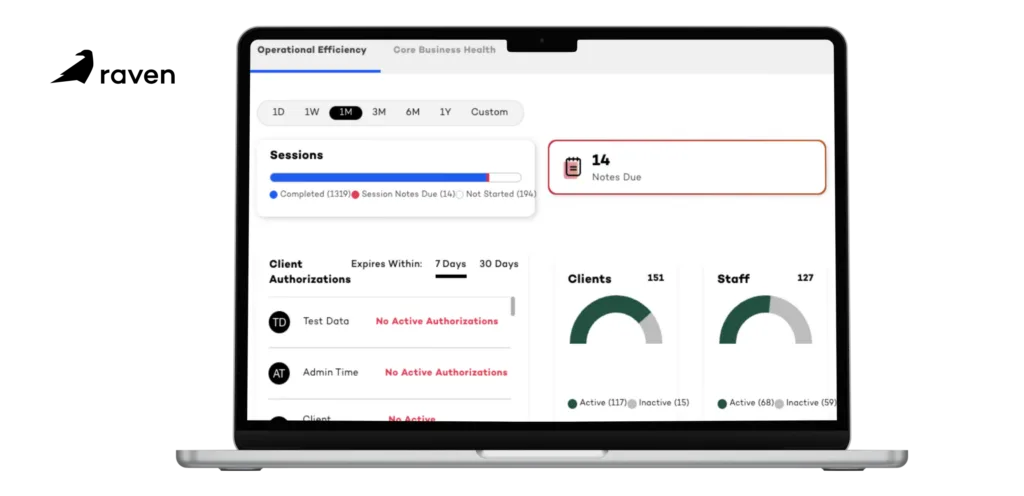
For leadership, Raven’s demo focuses on the big picture. You will see how the platform handles compliance, tracks authorizations, and protects your revenue cycle. The focus is on ROI and minimizing the unbillable hours your staff spends on administrative tasks. For a new clinic, pay particular attention to how the platform scales. What looks clean with five clients needs to still work when you expand and grow to fifty.
2. BCBAs and Clinical Supervisors
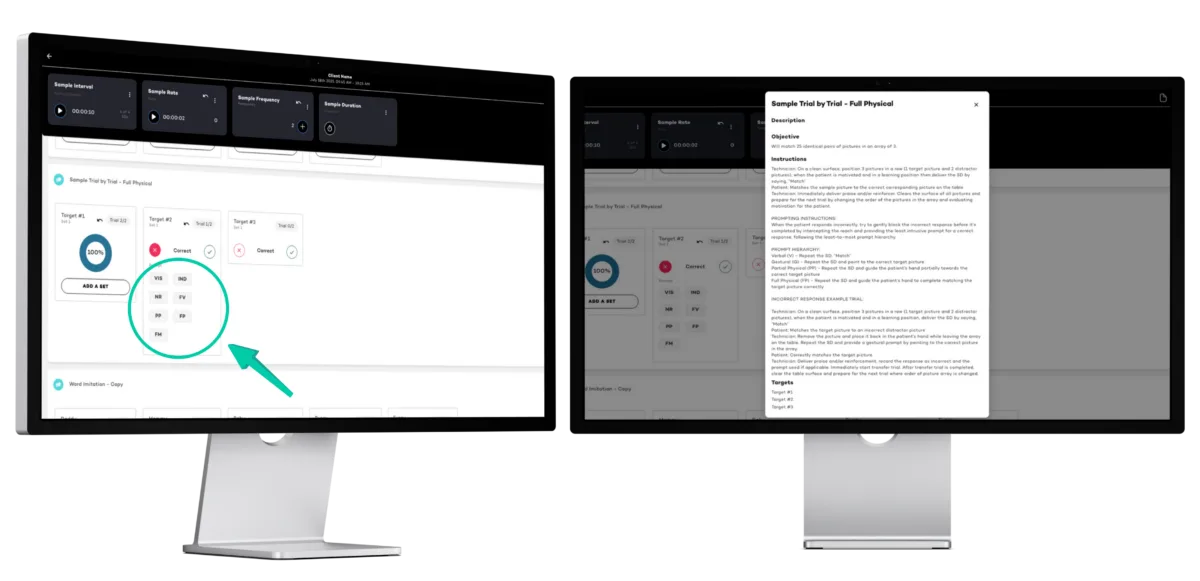
Clinicians care about the data, not the billing backend. During the demo, BCBAs will see how custom programming works, how standard and semi-logarithmic graphs are generated in real time, and how easily they can modify a learner’s target behaviors on the fly. If you are a new clinic owner who is also your own BCBA, this section of the demo will likely be where you spend the most time.
3. Administrators and RBTs
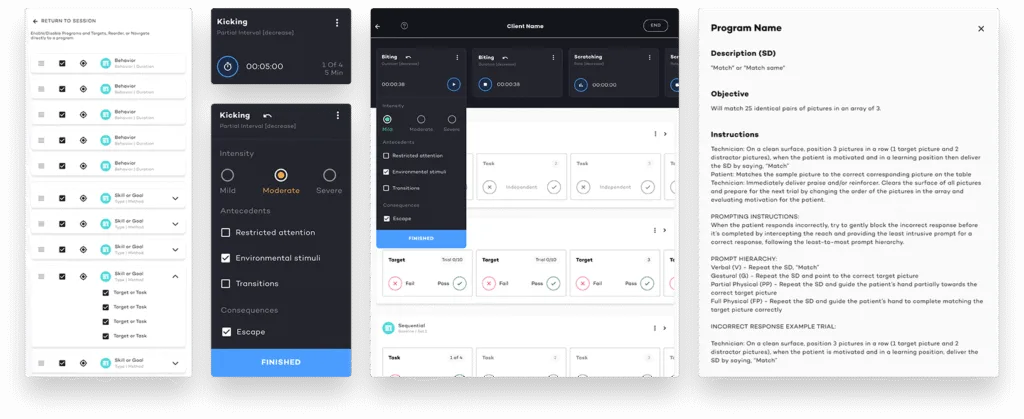
The unsung heroes of the clinic need to see the interface. For admins, the demo will highlight a typical day in the life, utilizing scheduling, reporting, and more. For the RBT perspective, the focus is pure usability: How many clicks does it take to record a prompt level?
For a brand new clinic, this is also a hiring and retention argument. Staff who are handed clunky software on day one form a negative first impression of your practice that is hard to reverse. A clean, intuitive RBT interface is something you can legitimately sell to potential new hires during interviews.
What to Look for In A Demo?
A strong demo won’t just list features; it will walk you through a day in the life of a therapy session. When looking at Raven Health, you will want to pay close attention to how the system handles the following critical areas:
1. The “Offline-First” Data Collection
This is arguably Raven Health’s biggest selling point, and it will be front and center in the demo. Most ABA software requires a constant internet connection. If the clinic Wi-Fi drops, or if an RBT is doing an in-home session in a dead zone, data is lost. Raven Health will discuss its offline capabilities; how an RBT can seamlessly collect frequency, duration, and interval data without an internet connection, which automatically syncs to the cloud the moment they are back online.
For a new clinic taking on in-home clients, this feature is not just nice-to-have, it is essential.
2. Intuitive Clinical Documentation
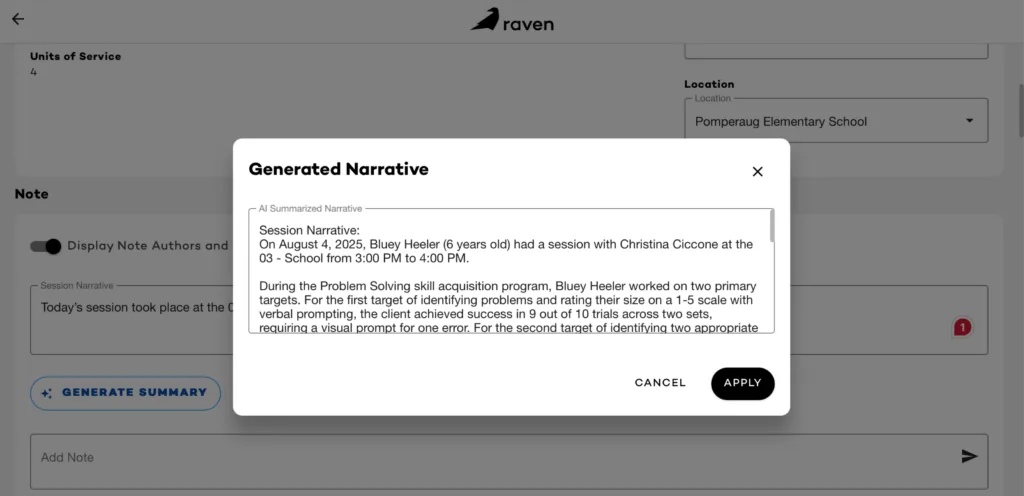
Session notes are a massive compliance hurdle. Raven’s demo will walk you through our integrated documentation system. You should ask to see how the software pulls raw session data directly into the final clinical note. This feature alone drastically reduces the time RBTs spend typing up summaries at the end of a session, ensuring that notes are accurate, compliant with insurance requirements, and completed before the staff member clocks out.
New clinics are disproportionately at risk for documentation audits because they have not yet established a track record with payers. Clean, auto-populated notes from day one are a form of protection. Ask the Raven team to show you what an audit-ready note looks like and how quickly it is generated.
3. Operational and Practice Management Support
Moving beyond the clinical side, the demo will pivot to operations. You will see how the scheduling matrix works; how to assign therapists to clients, manage cancellations, and track authorized hours so you never accidentally over-bill or leave money on the table. Pay attention to how the platform handles the transition from a completed schedule block directly into the billing and claims generation process.
For a growing clinic, cash flow is everything. The gap between delivering a session and getting paid for it can make or break your first year. Watch how quickly a completed session moves through the billing workflow in the demo, and ask what the average time to submission looks like for a new clinic getting started on the platform.
Assessing the Fit and Planning Your Next Steps
Watching a smooth presentation is one thing; visualizing it in your specific clinic is another. The primary goal of the demo is to answer one question: Will this actually make our lives easier?
As the demo wraps up, use the Q&A portion to ask hyper-specific questions about your current bottlenecks. If your biggest issue is parent training documentation, ask them to build a parent training goal right there on the screen. If you are worried about insurance credentialing timelines, ask how the platform supports that process while you are still getting paneled.
If you are pre-launch or in your first few months of operation, this Q&A is also a chance to understand what support looks like during onboarding. Ask directly: what does the first 90 days on the platform look like for a clinic that is just getting started? How much hand-holding is available, and what does it cost?
If you decide the platform is a potential fit, the next steps typically discussed include:
Data Migration: Ask exactly how your historical data, client demographics, and current behavior plans will be moved from your old system into Raven Health. If you are a new clinic with no legacy data, ask instead how initial client setup is handled and how long it typically takes to get a first client active on the platform.
Onboarding and Training: A new system is only as good as your staff’s ability to use it. Clarify what the training process looks like for your RBTs. For a new clinic still building its team, ask whether training guides can be used as part of your own staff onboarding process.
The Sandbox Phase: Many clinics request a limited sandbox account post-demo. This allows your lead BCBA to play around with the interface for a few days to ensure the clinical programming logic makes sense for your specific client base. For a new clinic, this is especially valuable because it lets you stress-test the system before you have real client data depend on it.
The Right Time to Evaluate Is Before You Need It
One of the most common mistakes new clinic owners make is waiting until they are overwhelmed before evaluating their software. By the time you are managing a full caseload, juggling credentialing, and onboarding new RBTs, you do not have the bandwidth to run a thorough demo process. You will end up defaulting to whatever is fastest rather than whatever is best.
Schedule your Raven Health demo while you still have the mental space to ask good questions, push back on the things that do not make sense, and think clearly about whether the platform matches how you intend to run your practice. The investment of one hour now can save you months of painful migration work later.
The clinics that get this right from the start are not the ones with the most resources. They are the ones that made deliberate decisions early, when it was still easy to change course.
Conclusion
Choosing a new practice management system is a heavy lift, but a well-executed demo strips away the marketing jargon and shows you exactly how the tool functions in the trenches. By knowing what to look for, you can make a decision that protects your clinicians’ time and your clinic’s bottom line.
When a family begins their journey with Applied Behavior Analysis (ABA), the focus is almost always on the child. We think about the hours of therapy, the Registered Behavior Technician (RBT) coming to the house, or the daily drop-offs at the clinic. But there is a silent engine that actually drives the long-term success of any ABA program: you, the parent.
ABA Parent Training isn’t just an add-on service or a mandatory box to check for insurance companies. It is the bridge between a child learning a skill in a controlled room and actually using that skill at the dinner table, in the grocery store, or at grandma’s house.
In this article, you will explore what ABA parent training involves and why caregiver involvement is critical for skill generalization and long-term progress.
Clinic Owner Note: Parent training is a billable service under most insurance plans (CPT codes 97156 and 97157). Beyond reimbursement, it’s one of your strongest levers for reducing early dropout; families who understand the “why” behind the work are far more likely to stay engaged through the full course of treatment.
What is ABA Parent Training?
Parent training is a coaching model. It transfers the tools of behavior analysis from the clinician’s hands into yours. It is not about turning you into a therapist; you are a parent first. Instead, it is about giving you a new lens to understand why your child does what they do.
The clinical term for this is generalization. Without parent involvement, generalization rarely happens effectively. Imagine your child learns to tie their shoes, but only when sitting in a specific blue chair at the clinic, and only when asked by their therapist. If they come home and can’t tie their shoes for you before school, have they really mastered the skill?
Parent training ensures that the progress made during therapy hours bleeds into real life.
Consistency is Key: Children with autism often thrive on predictability. If the clinic uses a specific visual schedule or a token economy to reward positive behavior, but home life is unstructured and reactive, the child receives mixed signals.
Skill Maintenance: Therapy eventually ends. Parent training equips you with the strategies to maintain those hard-won skills for years after discharge.
Reducing Stress: Understanding behavior functionally rather than emotionally, significantly lowers household stress levels. It moves you from reacting to behaviors to managing them proactively.
Goals, Strategies, and the “ABC” of Life
Many parents fear that training will be a lecture series where they are judged for their parenting style. In a quality ABA program, this couldn’t be further from the truth. Structured parent training is practical, data-driven, and highly individualized.
The ABC Model
One of the first things you will tackle is the “ABC” contingency. This is the heartbeat of behavior analysis.
Antecedent: What happened immediately before the behavior? (e.g., You said “time for bed.”)
Behavior: What exactly did the child do? (e.g., Threw the iPad.)
Consequence: What happened immediately after? (e.g., You negotiated for 5 more minutes to stop the crying.)
In training, you learn to spot these patterns. You might realize, “Oh, every time I give a warning about bed, he throws the iPad because it successfully buys him more time.” Once you see the pattern, you can change it.
Goal Alignment
Your Board Certified Behavior Analyst (BCBA) will sit down with you to identify socially significant goals. These aren’t just academic goals; they are survival goals for your family.
Do you need to be able to go to a restaurant without a meltdown?
Do you need your child to sleep in their own bed?
Do you need them to tolerate brushing their teeth?
These specific pain points become the curriculum for your training sessions.
For clinic owners, this goal-setting conversation is also a powerful retention tool. When parents see that the program is directly addressing the chaos in their daily life, not just running drills on a table, their buy-in skyrockets. Train your BCBAs to open every parent training relationship with this needs-based conversation.
Concrete Strategies
You will move beyond theory into actionable techniques such as:
Reinforcement: Learning the difference between a “bribe” (given to stop a bad behavior) and “reinforcement” (given to increase a good behavior).
Task Analysis: Breaking down complex chores like showering into tiny, teachable steps so you don’t have to nag.
Extinction: Learning how to safely ignore attention-seeking behaviors until they fade away, rather than accidentally feeding them.
A Collaborative Process- Empowerment, Not instruction
The best parent training feels like a partnership, not a classroom. You are the expert on your child; the BCBA is the expert on behavior. When these two expertise areas combine, magic happens.
This collaboration is designed to empower you. There is a specific kind of helplessness that comes from not knowing how to help your distressed child. Parent training replaces that helplessness with competence.
When a behavior occurs, you won’t freeze. You will have a plan. You will know, “Okay, this is an attention behavior. I know exactly what to do.”
Key aspects of this partnership include:
Feedback Loops: You try a strategy at home and report back. If it didn’t work, the BCBA doesn’t blame you; they tweak the plan.
Modeling: The clinician will often model the interaction with your child while you watch, then let you try while they provide supportive feedback.
Data Collection: You might be asked to take simple data (like tally marks on a sticky note) to track if a new intervention is working.
A note on staff training: The quality of your parent training program is only as strong as the BCBAs and RBTs delivering it. New clinic owners should invest in training their staff on how to coach adults, not just how to work with children. This is a distinct skill set, and one worth building into your onboarding and supervision protocols.
How to Build a Strong Parent Training Program at Your Clinic
If you’re in the early stages of building out your clinical services, here are some practical steps to ensure parent training is embedded, not bolted on:
Standardize your intake conversation. Every family should hear about parent training at the very first touchpoint, before authorization, before the initial assessment. Set the expectation that it’s part of the program, not an add-on.
Use consistent materials. Whether it’s a parent handbook, a shared visual schedule template, or a simple data sheet families take home, consistency in tools reinforces consistency in approach.
Track participation, not just delivery. Documenting that a parent training session occurred is the minimum. High-performing clinics also track caregiver comprehension, implementation fidelity at home, and goal progress, data your BCBAs can use to adjust the plan.
Address barriers proactively. Single parents, language barriers, work schedules, and caregiver burnout are all real obstacles to engagement. Build flexibility into your model, telehealth parent sessions, translated materials, or evening scheduling, so participation doesn’t quietly drop off.
Measure outcomes and share them. If you can demonstrate to a referring pediatrician or school district that families from your clinic are implementing strategies at home and seeing results, that’s a differentiator that no marketing campaign can replicate.
Conclusion
ABA Parent Training is about building a sustainable ecosystem for a child’s growth. It shifts the dynamic from “therapy is something that happens to my child” to “growth is something we do together.”
For the families you serve, this means more generalization, less regression, and stronger outcomes after discharge. For your clinic, it means families who understand and value the work, and are more likely to stay, refer others, and speak well of your program.
Parent training isn’t a checkbox. It’s one of the highest-leverage investments your clinical team can make: for the child, for the family, and for the long-term reputation of your clinic.
In the world of Applied Behavior Analysis, we are obsessed with data. We track frequencies, durations, and intervals to measure a client’s progress. But there is a hidden variable that often determines whether a child succeeds or stagnates, and it has nothing to do with the child’s behavior. It has everything to do with ours.
This variable is Treatment Fidelity also known as procedural integrity. In this article, you will explore what ABA therapy fidelity is and why consistent, accurate implementation of ABA programs is essential for client progress.
What is ABA Therapy Fidelity?
If ABA was to be considered a science, then the intervention is the medicine. For example, if a doctor prescribes 50mg of a medication, but the patient only takes 10mg, or takes it sporadically, or crushes it up when it should be swallowed whole, we cannot be surprised when the illness doesn’t go away. Treatment fidelity is ensuring the prescription is followed exactly as written.
At its simplest, Treatment Fidelity is the degree to which an intervention is implemented exactly as it was designed. It asks the question: Did the therapist follow the plan?
In an ABA session, this means:
Did the therapist deliver the reinforcement immediately (within 3 seconds) or did they wait too long?
Did they clear the field of distractors before placing the demand?
So, why is this non-negotiable? Because without high fidelity, our data is useless. If a child’s graph shows a “flatline” or a decrease in skill acquisition, we have to know why.
Scenario A: The teaching strategy is flawed and needs to be changed (The plan is the problem).
Scenario B: The teaching strategy is perfect, but it’s being taught inconsistent (The implementation is the problem).
If we don’t measure fidelity, we might mistakenly change a perfectly good behavior plan, thinking it didn’t work, when in reality, it was just never truly tested. This wastes valuable time; a resource our clients cannot afford to lose. High fidelity ensures that when a child succeeds, we know why. And when they struggle, we know exactly where to look to fix it.
Common Challenges Impacting Fidelity: The Human Factor
We have to be realistic; ABA is implemented by humans, not robots. And humans get tired, they forget things, and they bring their own habits into the session. Even the most well-intentioned Registered Behavior Technician (RBT) or parent can drift from the protocol.
1. Procedural Drift
This is the silent killer of ABA programs. Over time, a therapist might start cutting corners or adding their own flavor to a program. Maybe they stop using a visual timer because “he knows how long to wait now.” Slowly, the intervention morphs into something entirely different than what the BCBA wrote.
2. Staff Turnover and The Telephone Game
The turnover rate in human services is notoriously high. When a new therapist takes over a case, they often learn by watching the current therapist rather than reading the original plan. If the current therapist has “drifted,” the new therapist learns the drifted version. This creates a generation of staff implementing a diluted version of the therapy.
3. Overly Complex Protocols
Sometimes, the blame lies with the supervisor. If a behavior plan requires the therapist to track three different behaviors, deliver a token every 30 seconds, and use a complex correction procedure simultaneously, fidelity will drop. If the plan is too hard to do, it won’t get done.
4. Lack of Feedback
If an RBT is doing something slightly wrong like reinforcing a behavior too late and nobody corrects them, that error becomes a habit. Without eyes on supervision, bad habits calcify.
Impact of Training Systems
So, how do we fix it? We cannot just demand perfection; we have to build systems that support it. Ensuring fidelity is an ethical obligation under the BACB Ethics Code. We are promising effective treatment, and we can only deliver that through rigorous support.
The Solution is Behavioral Skills Training (BST). You cannot just hand a staff member a packet of papers and say, “Read this.” The gold standard for maintaining fidelity is Behavioral Skills Training.
Instruction: Explain the why and how of the procedure.
Modeling: The supervisor demonstrates the skill with the client while the RBT watches.
Rehearsal: The RBT practices (role-play) without the client first, then with the client.
Feedback: Immediate, corrective, and supportive feedback is given until the RBT is fluent.
Data-Driven Supervision
Supervisors should be collecting data on the therapist just as often as the therapist collects ABA data on the client. Using a Fidelity Checklist during supervision turns observations into structured ABA data collection. Instead of saying, “I don’t think you’re doing this right,” it becomes, “Step 4 on the checklist shows the prompt was missed; let’s practice it together.”
Visual Anchors
To combat drift, successful clinics use visual aids. Flowcharts, laminated protocol summaries on the wall, or quick “cheat sheets” on the data tablet help keep the correct procedure top-of-mind, reducing the cognitive load on the therapist.
Conclusion
Treatment fidelity is the bridge between the science of behavior analysis and the art of helping a human being. It requires humility from supervisors to write clear plans, and dedication from therapists to follow them.
When we prioritize fidelity, we aren’t just being sticklers for the rules. We are honoring the trust the family has placed in us. We are ensuring that every minute of therapy counts, giving the learner the absolute best chance to reach their potential.