by Raven Health | Dec 11, 2025 | Blogs
HIPAA (Health Insurance Portability and Accountability Act) is the U.S. law that protects patient health information. In an ABA clinic, everything from behavior charts to progress notes can be considered private health data. Choosing HIPAA-compliant software isn’t optional; it’s a legal and ethical must.
If client data leaks or is misused, your practice can face severe consequences. Beyond fines, a breach destroys trust with families. HIPAA compliance means protecting your clients and your clinic’s reputation. In this article, you will learn why HIPAA compliance is crucial for ABA practice.
Key Security Features to Look For
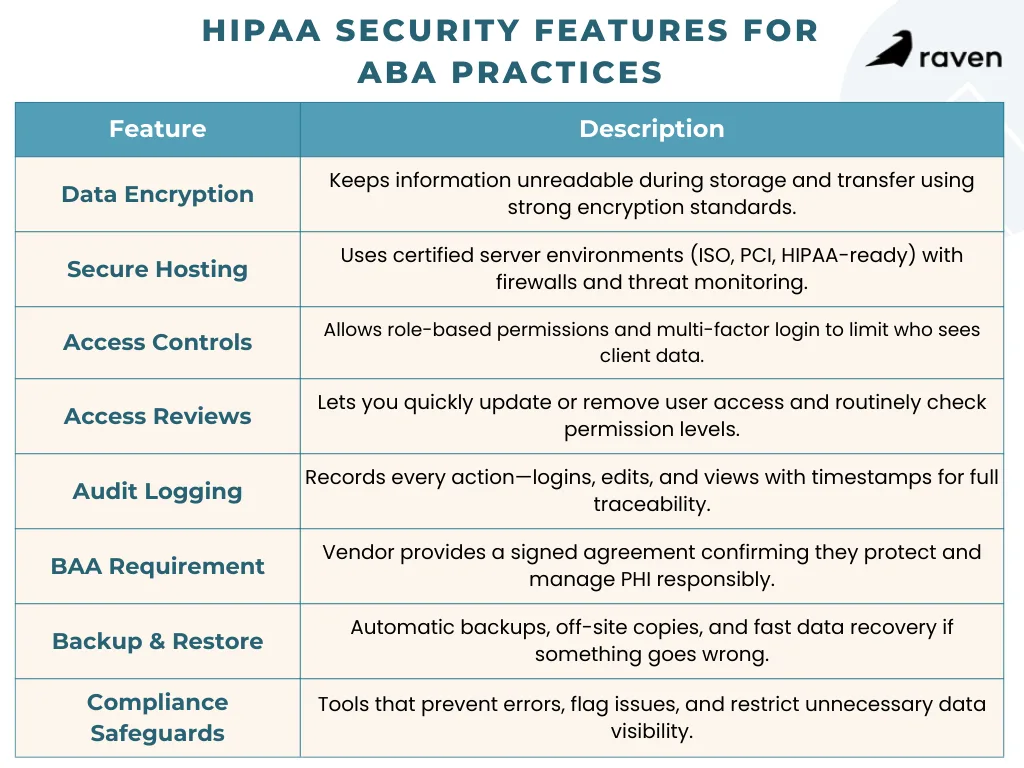
When evaluating ABA software, insist on built-in safeguards for protected health information (PHI). Here are the critical features and controls:
1. Strong Encryption
The software should encrypt data both at rest (when it’s stored) and in transit (when it moves over networks). Look for industry-standard encryption like AES-256. This scrambles data so attackers can’t read it even if they intercept it. For example, reputable services use 256-bit AES encryption on stored files and SSL/TLS for all web traffic.
2. Secure Hosting Standards
Check that the vendor’s servers meet recognized security standards (ISO 27001, PCI DSS, or HIPAA-ready cloud hosting). Data centers should use firewalls and intrusion detection and allow you to manage encryption keys if possible. A vendor compliance page or data sheet should mention these certifications or audits.
3. Access Controls & Authentication
The software must let you create user accounts with role-based permissions. For instance, a Registered Behavior Technician (RBT) should see only their assigned clients’ data, while a Board Certified Behavior Analyst (BCBA) or admin might have broader access.
Also require Multi-Factor Authentication (MFA); logging in should require more than just a password (such as a code from an app or text). These measures ensure that if a device or password is compromised, the attacker still can’t easily access PHI.
4. Regular Access Reviews
It should be easy to add or remove users and to review permissions. Good software lets you instantly revoke access when an employee leaves and quickly adjust roles as people switch jobs. Regularly auditing who can see what is a core HIPAA practice.
5. Comprehensive Audit Trails
Every action, including logins, data views, edits, and deletes, should be logged with a timestamp and user ID. HIPAA requires that you be able to prove what happened, when, and by whom. A compliant system will keep real-time logs of all activity.
This means if someone updates a behavior goal or enters session notes, that event is recorded immediately. You can then review the history during an internal check or external audit.
6. Business Associate Agreement (BAA)
Any vendor hosting or processing PHI must be willing to sign a BAA. This legal contract makes the vendor responsible for protecting your data. Never use software without a BAA. In fact, under HIPAA rules, the software provider is treated as a business associate and can be held directly liable for breaches. Always get the BAA in writing before you start using the system.
7. Automated Backups & Recovery
Confirm the system runs regular off-site backups and that data can be restored easily. Ideally, the vendor uses a “3-2-1” strategy (three copies of your data, on two types of media, with one copy offsite). Test the restore process. If there’s a ransomware attack or server failure, you must be able to recover quickly without losing weeks of client progress notes.
8. Built-In Compliance Features
Bonus points for ABA-specific safeguards. Some systems automatically flag or block errors. For example, good platforms might alert you if a clinician’s certification has lapsed, preventing billing for an unlicensed practitioner.
Others enforce minimum necessary rules so front-desk staff can schedule sessions without seeing clinical details. These workflow guardrails keep people honest without slowing them down.
Balancing Security with Usability
High security is crucial, but if the software is too rigid, clinicians may resort to unsafe workarounds (like shadow charting on paper). Conversely, a system that’s too careless risks missing data or unauthorized access. The best HIPAA-compliant ABA tools are designed to be secure by default but user-friendly.
Workflow Integration
Choose software that fits ABA workflows. For example, make sure mobile apps let therapists collect data in homes or schools and sync it immediately. Real-time sync means everything is logged right away, so nothing falls through the cracks.
Intuitive Role Use
When guardrails like role-based limits are built into the user interface, staff barely notice them. For example, a BCBA logging in might automatically see all supervisory data and the full patient record, whereas an RBT sees only their session programs and notes.
Parents or teachers accessing the portal see only their child’s progress. This keeps data safe without extra steps for users.
Offline Capability
Many ABA teams work on tablets or laptops without constant internet. Good HIPAA software caches the data offline and uploads it securely when back online. This way, therapists stay productive, and the audit trail is updated seamlessly once connected.
Compliance Built In
Look for features that enforce compliance quietly. For instance, automatic activity logs, timeout logouts, and encrypted local storage. The software should handle the hard parts (like encryption and logging) in the background so your staff can focus on therapy.
Conclusion
HIPAA compliance is critical for any ABA practice handling client data. The right software will shield sensitive information without getting in your way. At a minimum, look for AES-256 encryption, role-based access with multi-factor logins, audit logs that capture every action in real time, a signed BAA, and regular backups and recovery plans.
By carefully evaluating testing software in real workflows and confirming security measures, ABA practices can protect PHI, maintain compliance, and support efficient clinical operations.
Sources:
Encryption Best Practices for Protecting ePHI in the Cloud
HIPAA Compliance and Cloud Technologies: 5 Ways to Optimize Your Data Security
Enhancing HIPAA Compliance in the Cloud
Security Rule Guidance Material | HHS.gov
by Raven Health | Dec 10, 2025 | Blogs
Growing a new ABA practice means keeping an eye on the numbers. By regularly tracking key performance metrics, owners and clinicians get a clear picture of how well their programs and operations are working.
Data helps you spot problems early, make smarter decisions, and improve both client care and business health. In this article, you will learn some essential key metrics every new ABA practice should track.
1. Client Progress and Outcomes
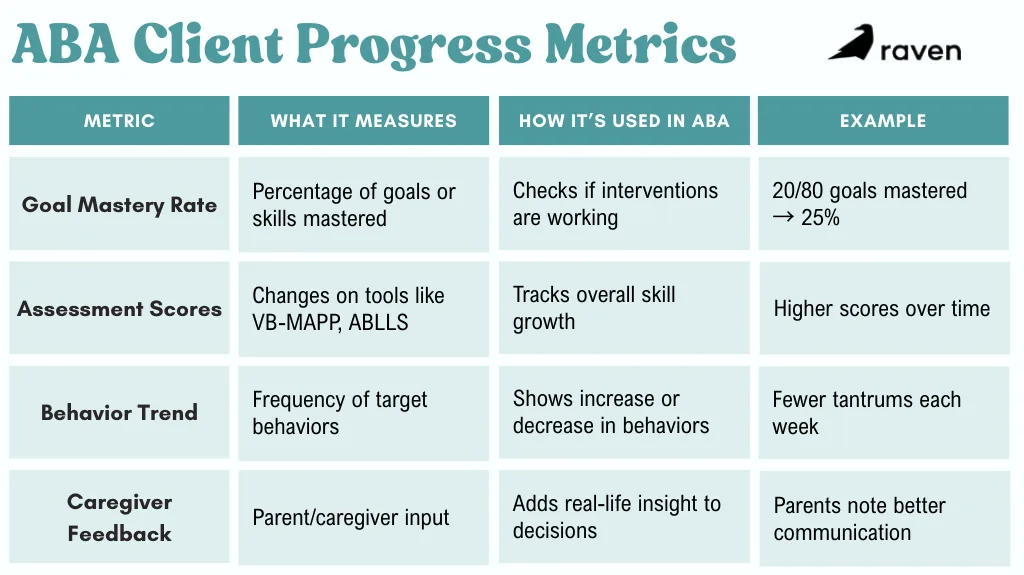
Measuring how clients improve is at the heart of ABA care. You can track skill acquisition and behavior goals by using standardized tools and visual charts.
For example, many practices count the percentage of treatment goals mastered each quarter or improvements on assessments.
If a child masters 20 out of 80 goals in three months, their progress rate is 25%. Trends like this show whether current strategies are working.
- Goal mastery rate is the percentage of behavioral goals or skills achieved over time.
- Assessment scores such as the changes on tools like the VB-MAPP or ABLLS assessments.
- Behavior trend is the count/frequency of target behaviors (e.g. tantrums) versus time.
- Caregiver feedback includes parent surveys on the child’s improvements and engagement.
These figures make growth concrete. For instance, if data show only 50% of goals are met, supervisors might adjust interventions or increase therapy hours.
Consistent tracking allows therapists to systematically assess progress and tweak plans as needed. This ensures each child’s program is truly effective and evidence-based.
2. Session Attendance and Retention
The best therapy plans only work if clients actually attend. Attendance rate (the percent of scheduled sessions that occur) is a must-watch metric. High attendance ensures consistency; missed appointments slow progress and shrink revenue.
- No-show/cancellation rate to track how many sessions are missed each month (e.g. 5 no-shows out of 100 sessions = 5%). Aim to keep this low (often under 5–10%).
- Turnover rate is the percentage of clients who end therapy early. Understanding why families leave (dissatisfaction, insurance, etc.) highlights service gaps.
- Referral and retention to monitor how many new leads convert to ongoing clients and how many complete recommended programs.
Improving attendance often involves reminders and flexibility. Setting up phone/text reminders or online scheduling can bump rates higher. By watching this metric weekly, you can quickly spot if one client or program needs outreach or if systemic issues (like scheduling conflicts) are causing gaps.
3. Staff Productivity and Utilization
A practice’s therapists are its greatest resource. Tracking how they’re used is crucial. Staff utilization rate measures the portion of employee hours spent in billable therapy versus non-billable time.
If a full-time RBT works 40 hours a week but only delivers 28 hours of client sessions, the utilization rate is 70%.
- Billable hours percentage is the total therapy hours delivered ÷ total available hours × 100.
- Sessions per therapist is the average number of sessions each therapist completes weekly.
- Case load is the number of active clients per BCBA or RBT.
- Overtime or idle time track extra hours or gaps in schedules.
Another approach is to measure session completion rate per staff member. For example, if a therapist is scheduled for 20 sessions in a week but completes only 18, that’s a 90% completion rate.
Monitoring these numbers helps managers balance workloads. If utilization is only 60%, you might hire more clients or cross-train staff. If it’s 95% (almost no breaks), you should hire or reassign tasks to prevent burnout.
4. Billing Accuracy and Financial Metrics
Money matters as much as therapy details. Accurate billing keeps your clinic financially healthy. Track the following finance-related metrics:
- Claim approval rate, which is the percentage of insurance claims paid on first submission.
- Average reimbursement time tracks the days between service date and insurer payment. Shorter is better. Long lag times can signal administrative bottlenecks.
- Claim denial rate is the portion of claims rejected. Every denied claim needs rework. Keeping this low (e.g., below 5–10%) is vital.
- Gross collection rate is the collected revenue ÷ billed charges × 100.
- Days in Accounts Receivable (AR) tracks how long it takes on average to collect an outstanding invoice. Fewer days means healthier cash flow (industry targets are often under 45 days).
By watching billing data, you can find errors early. For instance, if denial rates spike, it may mean documentation issues or coding mistakes.
Likewise, tracking the number of sessions billed versus delivered (the hours delivered vs. authorized KPI) ensures you aren’t leaving money on the table.
Finally, revenue per session is a useful gauge. Divide total revenue by total sessions to see how much each session brings in on average. If this number falls, it could hint at lower reimbursement rates or excessive discounts. Adjusting pricing or payer mix may be needed.
Conclusion
Collecting all these metrics does more than fill a spreadsheet; it drives better care and growth. Consistent tracking helps you spot trends and make informed choices. For example, if weekly data show one client’s progress slipping, you can intervene faster (add hours or adjust techniques). If staff utilization drops unexpectedly, you might investigate scheduling problems before revenue dips.
Using performance insights also ensures compliance and quality. Tracking metrics like authorization renewals and treatment duration keeps the practice aligned with insurance rules.
In short, a dashboard of ABA metrics empowers owners and clinicians to ask the right questions (“Why did attendance drop 10% this month?”) and test solutions. Over time, this feedback loop boosts both the quality of care and operational growth.

by Raven Health | Dec 9, 2025 | Blogs
ABA programs work best when professionals from different fields team up. In a multidisciplinary ABA team, Board Certified Behavior Analysts (BCBAs) work alongside speech therapists, occupational therapists (OTs), psychologists, educators, and parents.
This collaborative model covers all areas of a child’s development, such as communication, motor skills, social-emotional skills, behavior, and more, so nothing is missed. By aligning their expertise, the team creates holistic treatment plans and coordinated care that lead to better outcomes for clients. In this article, you will explore the benefits of multidisciplinary collaboration in ABA.
1. Holistic Treatment Planning
When a team collaborates, treatment planning becomes integrated. All professionals align their interventions so the child hears the same messages everywhere. For example, if an OT recommends a quiet corner to reduce sensory overload, the BCBA can incorporate that into behavior goals so the child stays calmer and can learn better. By sharing information, the team avoids mixed messages (for instance, one therapist telling a child to use one technique and another suggesting a different one).
Key elements of holistic planning include:
- Unified Goals: The team meets regularly to agree on priorities, for example, to improve requesting or manage frustration. Clear contracts or role agreements spell out who does what, preventing overlapping or conflicting strategies.
- Family Involvement: Families join team discussions and practice plans at home. When parents know the therapy targets and methods, they reinforce them throughout the day. This consistent home–school–clinic approach is family-centered and reduces confusion.
- Adaptive Planning: As the child grows, the team adjusts goals together. For example, a teenager’s plan might shift from basic communication to social skills for friendships, and the team all move forward on that new target.
Children receiving a combined program of ABA, speech, OT, etc., often make larger gains than those in isolated services. It is found that kids in integrated therapy achieve communication and social milestones more quickly than children receiving each therapy separately. This means a child may learn to speak their first words and use them socially faster when SLP goals and ABA techniques reinforce each other.
By coordinating, therapists avoid giving children too many different instructions. For example, visual schedules or reward systems can be shared across sessions. In short, holistic, team-based planning guarantees that no area is ignored.
2. Improved Communication and Coordination
Successful teams communicate clearly and frequently. Open dialogue and regular check-ins are key:
- Regular Meetings: Teams often schedule weekly or monthly meetings. In these sessions, therapists share progress data and discuss challenges in real time. This keeps everyone informed. For example, if an ABA session shows a new difficulty, the SLP or OT can quickly adapt their sessions.
- Shared Information: Many teams use shared notes, progress trackers, or apps so everyone sees the latest data. This transparency means a teacher or therapist can pick up on another’s strategies. Digital tools or written logs help make this process seamless.
- Role Clarity: From the start, defining each person’s role (often in writing) prevents confusion. When everyone knows who will target what skill, their efforts reinforce rather than contradict each other.
- Parent Communication: Keeping parents in the loop is part of team communication. Clear consent and information-sharing policies protect privacy and trust, but within those guidelines, families are treated as team members. Parents who understand the plan can ensure home practices match therapy.
Good communication directly improves outcomes. When an ABA therapist and an SLP, for example, use the same cues and reinforcements, skills learned in speech sessions are reinforced in ABA and vice versa. This consistency accelerates learning and makes behaviors stick. It also means therapies complement one another rather than clashing.
3. Shared Expertise
Pooling expertise means each professional can learn from the others and incorporate new ideas:
- For instance, an OT might train the BCBA in a deep-pressure strategy that calms the child, allowing ABA learning to happen more smoothly.
- Conversely, a BCBA might teach an SLP how to break language goals into small teachable steps.
- Psychologists and medical professionals can alert the team to co-occurring issues (like anxiety or sleep problems) that influence behavior, leading to a more informed ABA plan.
By working together, the team creates rich, multi-layered interventions. For example, if a child is learning to request help verbally, the SLP might use picture cards while the BCBA teaches the behavior of raising a hand.
The child then hears the same goal from two directions. This collaborative learning also keeps the program fresh and personalized, rather than formulaic.
4. Better Behavioral Outcomes
All these collaborative efforts translate into better results for the child:
- Faster Skill Acquisition: Children often reach milestones sooner. Integrated therapy means practice is reinforced in all settings.
- Generalization of Skills: When every team member teaches the same behaviors, children apply skills in new situations more easily. For example, a child learns to ask for a break with the ABA therapist, and the teacher and parents use the same words and signals, so the child uses the skill everywhere. This broad use of strategies comes from consistent teamwork.
- Reduced Conflicts: With a coordinated plan, caregivers don’t get conflicting instructions. Families report less stress when all providers speak the same language in treatment. Having one unified plan means no therapist is working at cross-purposes.
- Holistic Well-being: By addressing medical, sensory, social, and emotional factors along with behavior, the team treats the whole child. The end result is often a higher quality of life and better adaptive functioning.
Key Roles on an ABA Team
Each specialist brings unique skills to the team, ensuring every aspect of development is addressed:
Behavior Analysts (BCBAs)
They design and oversee the ABA program. BCBAs create individualized behavior intervention plans that teach social, communication, academic, and daily living skills. They use data-driven methods to encourage positive behaviors and reduce challenging ones
Speech-Language Pathologists (SLPs)
SLPs focus on communication and language. They work on speech sounds, vocabulary, and social communication, and may introduce tools like picture cards or speech devices. By improving functional communication, SLPs help children express needs and interact more successfully.
Occupational Therapists (OTs)
OTs address sensory processing, fine motor skills, and daily living tasks. They help children manage sensory sensitivities (for example, being bothered by noise or touch) and teach skills like dressing, feeding, or handwriting. Strong sensory regulation and motor skills support better learning during ABA sessions.
Psychologists
Psychologists work on emotional and behavioral health. They assess issues like anxiety or attention that may affect learning. By teaching coping strategies and social skills, psychologists support the child’s mental well-being, which in turn makes ABA progress smoother.
Educators and Parents
Teachers and special educators implement strategies in the classroom, aligning academic goals with therapy goals. Parents and caregivers are trained to reinforce techniques at home. This family involvement makes sure skills generalize to daily life and keeps everyone working towards the same targets.
Together, these professionals cover all developmental domains. The combined insights of BCBAs, SLPs, OTs, and others mean that therapy is truly well-rounded and person-centered.
Conclusion
Multidisciplinary collaboration is a cornerstone of effective ABA therapy. By bringing together BCBAs, speech and language therapists, OTs, psychologists, educators, and families, ABA programs ensure that no part of a child’s development is overlooked. Clear communication, shared goals, and mutual support mean therapy is consistent everywhere the child goes. This team approach produces holistic, person-centered care that research consistently links with better and faster learning.
Sources
The Role of Multidisciplinary Teams in Autism Support Programs
The Benefits of Multidisciplinary Collaboration in ABA Programs
The Benefits of Multidisciplinary Collaboration in ABA Programs
Multidisciplinary Teaming: Enhancing Collaboration through Increased Understanding

by Raven Health | Nov 20, 2025 | Blogs

ABA data collection software turns complex therapy records into clear insights. Therapists need to gather accurate information about behaviors and skills. Good software helps teams log session data quickly, so they can adjust treatment and see real progress.
Studies show that clinics using consistent digital data collection make 35% faster progress toward goals than those relying on manual methods. In this article, you will explore the top features to look for in ABA data collection software.
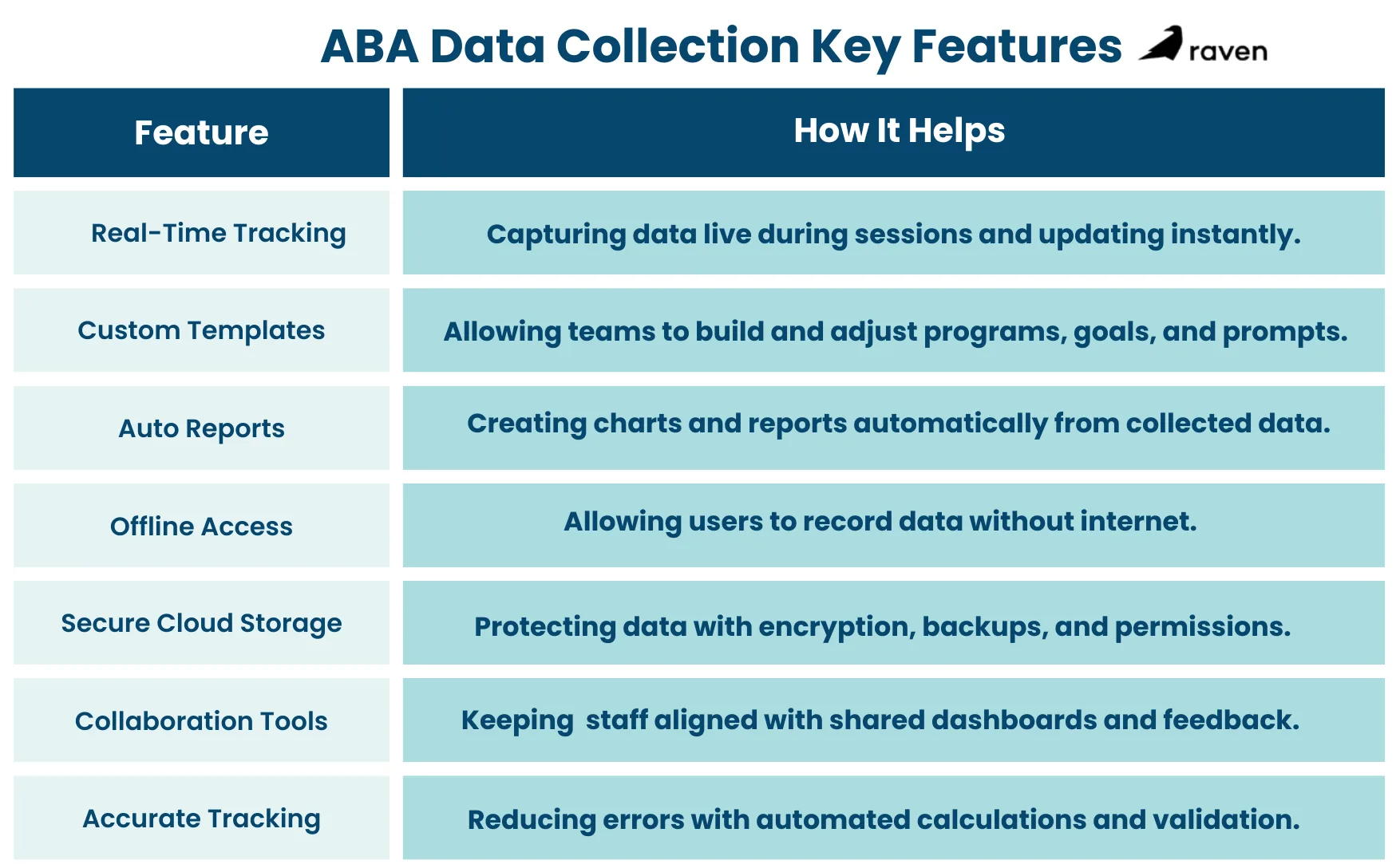
1. Real-Time Data Tracking and Entry
Live Session Recording
The best ABA apps let staff record data during therapy sessions on tablets or phones. This way, behaviors and trials are logged as they happen, not hours later from memory. A mobile app with auto-sync ensures no data is lost and that supervisors see updates right away.
Immediate Syncing
When data syncs in real time, BCBAs can access fresh information instantly. Real-time tracking frees clinicians from jumping between disjointed charts and saves time so they can focus on clients. This instant data flow helps teams spot issues quickly and adjust plans on the spot.
Accurate Behavior Logs
Entering data as it occurs cuts down errors, and digital timers and counters automatically calculate duration or frequency. This approach helps keep every data collection method consistent across staff and sessions, ensuring accuracy because even small mistakes can skew treatment decisions.
2. Customizable Programs and Templates
Editable Data Fields
It’s essential for ABA software to empower therapists to create fully customizable program templates. Clinicians can set up goal-specific data forms and fields for each child’s needs. For example, they can define unique prompts and goal steps in the system. This flexibility means the software fits the therapy, not the other way around.
Behavior and Skill Templates
Many platforms include built-in tools for common ABA program types. Users can generate templates for things like discrete trial training or preference assessments and adapt them to each case. This avoids recreating forms from scratch and keeps data collection consistent.
Integrated Session Notes
Custom program templates often tie into note-taking features. Providers can attach instructions or criteria to each data field. This ensures any therapist using the program knows exactly what to do and how to score each trial. Over time, having precise, standardized templates helps supervisors check consistency across staff.
3. Automated Reporting and Progress Visualization
Auto-Generated Reports
Good ABA data collection software can build progress reports and charts at the push of a button. Instead of manually compiling graphs, the system pulls together all the data for each goal. AI-powered tools can even auto-write session summaries that align with insurance requirements, saving clinicians hours of paperwork.
Built-in Charting
Software usually includes graphing tools that update as new data comes in. For example, one platform offers up to 20 customization options for progress graphs, you can add trend lines, split data by therapist, compare conditions, and more. These visual charts make it easy to see if a child is making gains or needs extra help.
Export and Review
It should be easy to export data and reports (PDF, CSV, etc.) for review outside the app. These visual reports help therapists, supervisors, and families understand progress without reading raw spreadsheets. Having ready-made graphs and summaries means everyone can stay informed at a glance.
Goal Mastery Features
Some software even automates mastery criteria. Clinicians can set targets (like “90% correct over three sessions”), and the system will flag or master out a skill once met. This automatic progress tracking cuts down on manual checks and ensures goals are updated promptly.
4. Offline Data Entry and Mobile Access
Offline-Mode
Therapists often work where the internet is spotty. Leading ABA apps let them record data offline and sync later. The app stores entries securely on the device until Wi-Fi returns. This way, a session isn’t interrupted by a network glitch, and once online, the data updates automatically, so nothing is lost.
Cross-Device Flexibility
Quality ABA software works on phones, tablets, and computers. Whether staff bring an iPad or a laptop, data goes into the same cloud system. This flexibility lets clinicians choose the device they’re comfortable with and ensures the entire team always sees the latest data.
Data Security Offline
Even in offline-mode, data stays encrypted on the device. When syncing later, it moves to the cloud over an encrypted connection. This protects client privacy without sacrificing the convenience of mobile data entry.
5. Secure Cloud Storage and Data Security
HIPAA-Compliant Cloud
All client data should be encrypted and stored on secure cloud servers. Reputable ABA software meets HIPAA standards, using encryption and access controls to safeguard information. This not only protects records but also ensures clinics stay compliant with privacy laws. (For example, one case study highlights how secure cloud storage reduced data loss for a clinic.)
Automatic Backups
Cloud-based systems automatically back up data, reducing the risk of loss if a device breaks or a file is deleted. Daily or real-time backups mean you don’t have to worry about losing months of data to a computer crash. One ABA platform even notes that secure cloud storage cuts down data loss dramatically.
User Permissions
Good ABA tools let administrators assign roles (BCBA, RBT, admin, etc.), so each team member sees only what they need. Audit logs track who entered or changed data, adding transparency. These security features help supervisors trust the data and protect sensitive client information.
6. Supervision and Collaboration
Shared Dashboard
Supervisors and team members work from one central database. A shared dashboard or client portal means therapists, BCBAs, and even parents can view the same data.
Real-Time Oversight
Because data is entered live, supervisors can review session data quickly. Clinical leads can monitor progress during or right after sessions. This immediate feedback helps them coach staff and ensure data quality in real time.
Built-In Communication
Many platforms include tools for notes or comments. Supervisors can add feedback directly in a session report, or therapists can flag unusual incidents. Keeping these messages linked to the client’s record avoids miscommunication. It’s like having a built-in chat about the data so nothing falls through the cracks.
Family Involvement
Sharing progress with parents improves collaboration. Some software lets providers share read-only reports or charts with families. When parents see clear evidence of success (or challenges), they can help reinforce skills at home. In this way, data collection becomes a team effort supporting the child.
7. Ensuring Accurate, Efficient Tracking
Error Reduction
Digital data entry dramatically cuts human mistakes. One ABA practice reported doubling data accuracy after switching from paper. On a digital form, counts and times add up automatically, and drop-down choices keep entries standardized. This means the data your team relies on is far more likely to be correct.
Consistent Measurement
The software enforces consistent methods (e.g., all staff use the same behavior definitions and units). This consistency is crucial for comparing data across sessions or staff members. If everyone records data the same way, progress graphs are reliable, and no one needs to second-guess whether a change in numbers is real or just an input error.
Built-In Calculations
Leading tools auto-calculate rates, percentages, and other metrics. For example, you might just enter trial outcomes, and the system shows you the percentage correct instantly. This saves time and keeps the team on task, rather than scrambling with calculators during a session.
Quick Alerts
Look for software that can flag data trends. For instance, if a child’s performance suddenly dips or if data hasn’t been entered for a while, the system can alert supervisors. These proactive checks help catch issues early and keep interventions on track.
Conclusion
Choosing the right ABA data software means weighing these features carefully. Look for tools that support live data entry, flexible program templates, automatic reporting with visual charts, offline/mobile access, and robust security. These capabilities not only save therapists time but also ensure every data point is reliable. They turn raw numbers into clear insights, driving better care.

by Raven Health | Nov 19, 2025 | Blogs

Momentary Time Sampling (MTS) is a practical method for collecting behavioral data in Applied Behavior Analysis. It tells you whether a target behavior may be happening at specific moments rather than recording everything that happens across an entire observation period.
This makes MTS fast, reliable for trends, and especially useful in group or busy settings. In this article, you will explore more about MTS, know how it differs from partial and whole interval recording, and learn its uses in ABA.
What is Momentary Time Sampling?
Momentary Time Sampling is a data collection method that involves observing at predetermined moments and recording whether the behavior is present exactly at that instant.
It works in the following ways:
- You divide an observation session into equal-length intervals (for example, twenty 30-second intervals during a 10-minute observation).
- At the end (or start) of each interval, you look up and mark whether the behavior is occurring at that moment.
- Count the number of “yes” checks and divide by total moments observed to get a percentage (moments with behavior ÷ total moments × 100).
MTS will provide you with a snapshot series, many quick photos of behavior across time, rather than a continuous movie, making it a practical tool for ABA data collection.
How to Conduct a Momentary Time Sampling Session?
Define the behavior clearly
Make it observable and measurable. For example: On-task behavior = eyes on work and hands engaged with materials.
Choose observation length and interval
Common choices include 10–30 minutes total and intervals of 15–60 seconds. Shorter intervals catch faster behaviors better. For example: 10 minutes with 20 thirty-second intervals.
Decide the moment to observe
Most practitioners use the end of each interval (e.g., at 0:30, 1:00, 1:30). This is simple and consistent.
Use a timer or app
Set an audible timer or an interval timer app that beeps at each moment to mark.
Record at each moment
Mark “1” if the behavior is present at the instant, “0” if not.
Calculate percent occurrence
% = (number of yes marks / total intervals) × 100.
Check reliability
Have a second observer collect data simultaneously during at least some sessions to compute Interobserver Agreement (IOA).
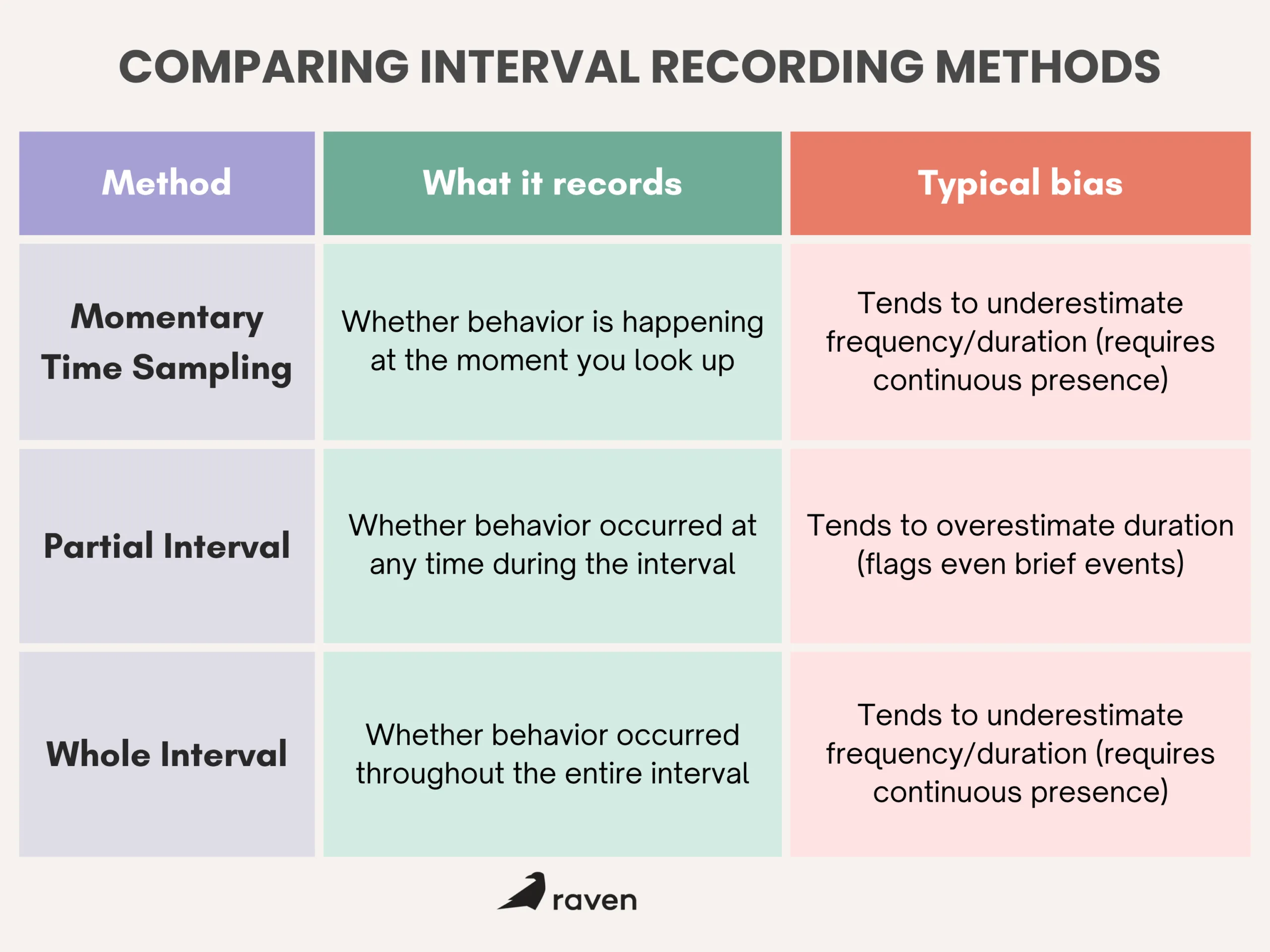
How MTS Differs from Partial and Whole Interval Recording?
- Partial interval says “yes” even if the behavior happened briefly; it inflates time estimates.
- The whole interval requires the behavior to last the full interval; it gives conservative (low) estimates.
- MTS is the middle ground: it samples at moments and is efficient, but it can miss events that occur between moments.
When is Momentary Time Sampling most useful?
Use MTS when:
- You are observing groups (classroom, therapy group), and a single observer can’t track every child continuously.
- Behaviors are high-frequency or occur many times a session, and counting every event is impractical.
- You want a quick trend measure to see whether behavior is increasing or decreasing across sessions.
- You need efficient data during community activities or natural settings where continuous recording is not feasible.
Some practical examples include:
- Measuring how many students are on-task during a 20-minute lesson (one observer can scan the group at each moment).
- Tracking hand-flapping in a classroom where it happens often. MTS gives a workable estimate without nonstop counting.
- Observing engagement at a community outing where staff must also supervise safety.
Benefits of Momentary Time Sampling
- Efficient: Requires less continuous attention than continuous recording, so it works well when observers have multiple responsibilities.
- Good for trends: Repeated MTS sessions quickly show whether a behavior is increasing or decreasing.
- Feasible in groups: One observer can collect data on multiple people by scanning at moments.
- Easy to train: Staff learn to look at specific moments and make a single yes/no judgment; this lowers training time.
- Reduced data volume: Less data to store and analyze than continuous methods, but enough to guide decisions.
Limitations of MTS and How to Reduce Them?
A few common limitations for MTS are as follows:
- MTS misses behavior between moments. If a behavior happens briefly between checks, MTS won’t catch it.
- Variable accuracy depending on interval length. Long intervals reduce accuracy for fast behaviors.
- It results in potential bias. Depending on when the moments fall, MTS can over- or underestimate real occurrence.
How to reduce problems?
- Use short intervals for fast behaviors (15–30 seconds). For slower behaviors, 30–60 seconds can be fine.
- Run pilot sessions comparing MTS with continuous recording on the same behavior to estimate bias.
- Train observers with video practice and use simultaneous IOA checks (aim ≥ 80% agreement).
- Occasional spot-checks with continuous recording help validate your MTS results.
- Interobserver Agreement (IOA) and data quality are essential with any sampling method. For MTS:
Have two observers record at the same moments and compute percent agreement: (agreements ÷ total moments) × 100. Check IOA regularly during training and periodically afterward. If IOA drops, review definitions, timing, and observer procedures, and retrain as needed.
Conclusion
Momentary Time Sampling is a simple, efficient way to collect useful behavioral data when continuous recording isn’t practical. It’s best suited for group settings, busy clinics, and high-frequency behaviors where full-event recording would be too hard. With clear definitions, short intervals, careful observer training, and periodic validation, MTS gives dependable trend data that supports good clinical decisions.
by Raven Health | Nov 14, 2025 | Blogs
Starting an ABA practice is exciting and full of practical pitfalls. Many new clinics stumble on the same issues that slow growth, hurt cash flow, or risk compliance. In this article, you will explore the most common mistakes that clinics make and practical steps to avoid them.
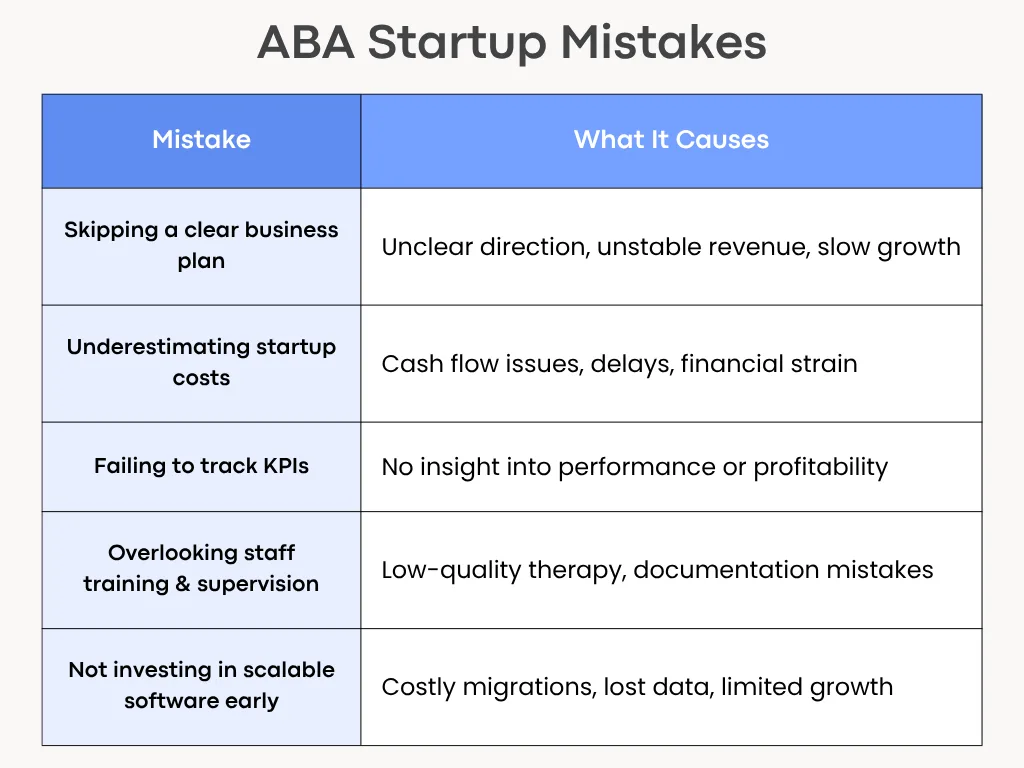
1. Skipping a Clear Business Plan
A good therapy model and strong clinical skills aren’t enough when starting an ABA practice. Without a written business plan, you won’t know who your clients are, how you will get paid, or when the clinic becomes profitable.
What to include in a simple plan?
- Mission and services: Who you serve (age, needs) and which services (intensive ABA, school consultation, tele-health).
- Market and referral sources: schools, pediatricians, insurance panels, and parent groups.
- Revenue model: Typical session rates, payer mix (private pay vs insurance), and expected caseload per clinician.
- Staffing plan: Roles and hires for year 1 and year 2.
- Financial projections: Monthly cash flow forecast for 12 months, break-even date.
- Growth milestones: When to add clinicians, an admin, or a second location.
Write a short one-page plan first and refine it after three months of operations. It’s far easier to adjust a written plan than to improvise under cash pressure.
2. Underestimating Startup Costs
Many founders count only rent and a computer. They miss recurring costs and one-off builds, so cash runs out before the practice stabilizes.
Costs people forget
- Credentialing deposits and payer enrollment fees.
- Billing software, clearinghouse fees, and EMR subscriptions.
- Staff recruitment, background checks, and credential verification.
- Training materials and initial supervision hours for BCBAs.
- Insurance (general liability, professional liability), office supplies, and marketing.
- Working capital to cover payroll for 3–6 months.
Build a conservative budget that includes a three-to-six-month cash buffer. When in doubt, overestimate costs and delay discretionary purchases until revenue is steady.
For more insights, check out our article on ABA startup costs to consider.
3. Delaying Credentialing and Insurance Setup
Credentialing with insurance companies and Medicaid can take months. Waiting to start creates a cash gap and slows patient access.
What to handle early?
- Start payer enrollment as soon as you choose your legal entity and NPI.
- Check state Medicaid requirements and EVV rules if you will bill Medicaid.
- Collect documents up front: provider licenses, malpractice limits, CVs, and contract signatures.
Begin credentialing 90–120 days before you plan to see your first insurance clients. Use a checklist to track submissions and follow-ups weekly.
4. Relying on Paper-Based Data Collection
Paper sheets result in slow supervision, transcription errors, and complicated billing. They also make remote work and audits harder.
Risks of paper
- Lost or illegible session notes.
- Extra admin time to enter data into billing or clinical systems.
- Poor data fidelity for clinical decisions.
Move to a basic digital data-capture tool from day one, even a simple app that syncs to CSV exports. Choose software that supports offline use if you do home visits. Train RBTs on consistent coding and make spot-checks part of supervision.
5. Ignoring Compliance and HIPAA Requirements
HIPAA and state privacy rules are non-negotiable. Gaps expose clients to risk and the clinic to legal and financial trouble.
Key compliance basics
- Sign Business Associate Agreements (BAAs) with any vendor that handles PHI.
- Use encrypted email or a secure portal for families.
- Limit PHI access by role and enable audit logs.
- Keep a breach response plan and test it.
Get BAAs signed before sharing client data. You can use a password manager and MFA for all staff accounts. Also, train staff on privacy rules during onboarding and yearly.
6. Using Disconnected Tools for Billing and Scheduling
Separate systems for scheduling, billing, and charting create manual handoffs, duplicate entry, and missed claims.
Consequences of using disconnected tools
- Billing delays and higher denial rates.
- Frustrated staff who spend time reconciling calendars and notes.
- Hard-to-run reports for utilization or payroll.
Choose an integrated practice management system that fits your budget and workflow. If you can’t afford an all-in-one yet, pick tools with good export/import or API connections and document manual steps to avoid errors.
7. Overlooking Staff Training and Supervision
Good hires aren’t ready without structured onboarding. Undertrained staff make documentation errors and deliver inconsistent therapy.
Elements of strong training
- Role-specific onboarding checklists (RBTs, BCBAs, admin).
- Shadowing and supervised practice blocks before independent caseloads.
- Regular fidelity checks and weekly supervision with documented feedback.
- A clear escalation path for clinical and behavioral emergencies.
Budget for at least 40–80 hours of training per new RBT in the first three months. You can use recorded role-plays and short quizzes to check understanding.
8. Failing to track Key Performance Indicators (KPIs)
Without KPIs you’re guessing whether the business or clinical work is succeeding. Small problems quickly become big.
KPIs to track from day one
- Financial: Days in Accounts Receivable (AR), claim denial rate, net collection rate.
- Clinical: Client attendance rate, average hours per client, and treatment progress by goal.
- Operational: Staff turnover, fill rate for open slots, average time to credential a provider.
Review a short KPI dashboard weekly and a report monthly. Use small experiments (change one thing at a time) and watch the metric move.
9. Neglecting Parent Communication & Collaboration
Parents are partners in therapy. Poor communication hurts retention, progress, and referrals.
What do parents need?
- Clear intake steps and timelines.
- Regular updates: brief weekly notes and a monthly progress snapshot.
- Simple ways to ask questions: portal messages, short phone office hours, or scheduled family meetings.
Send a one-page welcome packet with the treatment plan, goals, who to contact, and what to expect in the first 90 days. Ask for feedback at 30 and 90 days.
10. Not Investing in Scalable Software Early On
Buying the cheapest software that doesn’t scale forces painful migrations later. Data exports, retraining, and process rework cost time and money.
Signs your software won’t scale
- No offline data capture for in-field staff.
- Limited reporting or no API for payroll and billing.
- Difficulty exporting client records in usable formats.
Choose a scalable software like Raven Health that covers core needs (data collection, scheduling, billing, and reporting). Moreover, prioritize exportability and vendor willingness to assist with migration. Consider total cost of ownership, including migration and not just license price.
Conclusion
Many early ABA clinic problems are avoidable with simple, practical planning. Build a short business plan, budget realistically, start credentialing early, and pick scalable digital tools. Train staff well, track key metrics, and keep families part of the process. These steps reduce stress, speed cash flow, and let clinicians focus on what matters most: delivering good care.